Points
-
Upper airway injuries are due to thermal burns from heat transfer, while lower airway injuries are secondary to chemical and particulate irritants.
-
Airway edema, carbonaceous sputum, soot in the nares or oropharynx, facial burns, and singed nasal hairs all indicate potential inhalation injury.
-
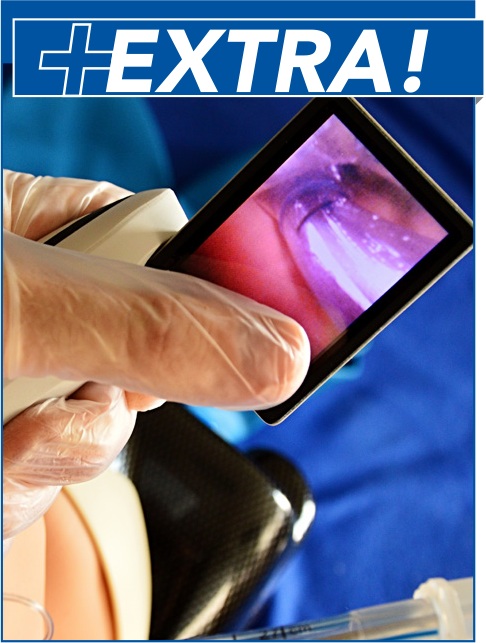
The diagnosis and prognostication of the course of inhalation injury is challenging, since much of the damage is not visible upon initial presentation.
-
A complete physical examination, including a primary and secondary survey, is essential to rule out other acute injuries.
-
Pulse oximetry may be falsely normal despite significant carbon monoxide (CO) poisoning.
-
Check a glucose fingerstick, lactic acid level, troponin, pregnancy test, and a chest x-ray in all smoke inhalation victims.
-
Consider obtaining an electrocardiogram if there is concern for CO exposure, since CO toxicity increases the risk of dysrhythmias and myocardial ischemia.
-
A venous blood gas may be used in lieu of an arterial sample to determine a carboxyhemoglobin level. Levels correlate loosely with symptoms.
-
An elevated lactic acid level in a smoke inhalation victim should raise concern for cyanide toxicity.
-
Checking a cyanide level is not recommended for management in the ED.
-
Consider a trial of noninvasive positive-pressure ventilation for patients with mild symptoms and no contraindications.
-
The use of hyperbaric oxygen therapy for CO poisoning is controversial and remains a Level B recommendation. Normobaric 100% FiO2 remains the standard of care.
-
Bronchodilators, inhaled epinephrine, inhaled nitric oxide, inhaled heparin, inhaled N-acetylcysteine, and inhaled anticoagulants may all play a role in managing patients with smoke inhalation injuries. Further studies are needed.
-
Mechanical ventilation is an independent predictor of mortality and can also worsen lung injury.
-
Pneumonia and acute respiratory distress syndrome (ARDS) are both common complications of inhalation injury.
-
Up to 33% of burn patients require intubation. Of those, 33% to 54% develop ARDS.
-
All patients for whom there is concern for potential inhalation injury should be closely observed in a monitored setting for 24 hours, with a low threshold for intubation.
-
The presence of inhalation injury is one of the American Burn Association criteria for burn center referral.
Click here to read the full issue!
Pearls
-
For suspected cyanide poisoning, hydroxocobalamin 5 g IV should be administered immediately.
-
Caution must be used when resuscitating smoke inhalation patients, as over-aggressive IV fluids can worsen airway edema.
-
There is no conclusive evidence supporting the use of corticosteroids to reduce airway edema in smoke inhalation victims.
-
Endotracheal intubation is indicated for patients with deep burns to the face and neck, blistering or edema of the oropharynx, hoarseness or stridor, or large cutaneous burns greater than 40% of total body surface area.
Table 1. Classification of Inhalation Injury
.JPG)
Access more tables and figures here

MDCalc Score Calculators
Radiologist’s Score for Inhalation Injury:
Abbreviated Injury Score Calculator:
Reader Comments
Last month’s issue was on Thermal Burns. (
www.ebmedicine.net/Burns) When we asked, “What changes do you anticipate making in your practice as a result of this activity?” your colleagues said:
-
Use initial cool water therapy and provide more evidence to my colleagues to stop using silver dressings on wounds.
-
Use the Lund & Browder chart when I can.
-
Pay more attention to clinical parameters and urine output when assessing fluid needs.
-
Use lactated Ringer’s instead of normal saline.
-
I now have a better idea of when I should consider transfer to a burn center and indications for emergent treatment prior to transfer.
Most Important References
-
Walker PF, Buehner MF, Wood LA, et al. Diagnosis and management of inhalation injury: an updated review. Crit Care. 2015;19:351. (Review) DOI: https://doi.org/10.1186/s13054-015-1077-4
-
Sheridan RL. Fire-related inhalation injury. N Engl J Med. 2016;375(5):464-469. (Review) DOI: https://dx.doi.org/10.1056/NEJMra1601128
-
1Enkhbaatar P, Pruitt BA Jr, Suman O, et al. Pathophysiology, research challenges, and clinical management of smoke inhalation injury. Lancet. 2016;388(10052):1437-1446. (Review) DOI: https://doi.org/10.1016/S0140-6736(16)31458-1
-
Weaver LK. Clinical practice. Carbon monoxide poisoning. N Engl J Med. 2009;360(12):1217-1225. (Review) DOI: http://dx.doi.org/10.1056/NEJMcp0808891
-
Buckley NA, Juurlink DN, Isbister G, et al. Hyperbaric oxygen for carbon monoxide poisoning. Cochrane Database Syst Rev. 2011Apr 13(4):CD002041. (Systematic review; 6 trials, 1361 patients) DOI: https://dx.doi.org/10.1002/14651858.CD002041.pub3
-
Wolf SJ, Maloney GE, Shih RD, et al. Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with acute carbon monoxide poisoning. Ann Emerg Med. 2017;69(1):98-106. (ACEP Clinical Policy) DOI: https://doi.org/10.1016/j.annemergmed.2007.10.012
To Read The Companion Article:
To Read The Companion Article:
To Read The Companion Article:








 678-366-7933
678-366-7933