Table of Contents
When treating patients who have suffered injury in a fire, managing their airway is as critical as treating their burns. Following on the February 2018 issue on Thermal Burns, this issue reviews strategies for diagnosing and treating inhalation injuries in fire-exposed patients.
How is inhalation injury severity measured?
What are the differences between injury to the upper airway, the lower airway, and systemic effects of intoxication?
What are the signs of carbon monoxide and cyanide poisoning, and what are the best treatments?
What kind of diagnostic tests should be done, and what will they tell you?
Blood gas, CO-oximetry, pulse oximetry, and pulse CO-oximetry: when should they be used and when might they be falsely normal?
What are the benefits and limitations of CT, bronchoscopy, and laryngoscopy?
Are prophylactic antibiotics warranted to prevent pneumonia?
What are the optimal methods of airway management when edema and airway obstruction is a threat?
-
Abstract
-
Case Presentations
-
Introduction
-
Selected Abbreviations
-
Critical Appraisal of the Literature
-
Etiology and Pathophysiology
-
Upper Airway Thermal Injury
-
Lower Airway and Lung Parenchymal Injury
-
Systemic Cellular Dysfunction of Carbon Monoxide and Cyanide Exposure
-
Differential Diagnosis
-
Prehospital Care
-
Emergency Department Evaluation
-
History
-
Physical Examination
-
Diagnostic Studies
-
Blood Gas and CO-Oximetry
-
Pulse Oximetry
-
Noninvasive Pulse CO-Oximetry
-
Lactic Acid
-
Cyanide Testing
-
Other Laboratory Testing
-
Electrocardiogram
-
Chest X-Ray
-
Chest Computed Tomography
-
Fiberoptic Bronchoscopy
-
Limitations of Fiberoptic Bronchoscopy
-
Direct and Fiberoptic Laryngoscopy
-
Other Clinical Testing
-
Treatment
-
Airway Management
-
Medical Adjuncts
-
Treatment for Carbon Monoxide Poisoning
-
Treatment for Cyanide Poisoning
-
Complications
-
Special Populations
-
Pregnant Patients
-
Geriatric Patients
-
Controversies and Cutting Edge
-
Extracorporeal Membrane Oxygenation
-
Point-of-Care Ultrasound
-
Disposition
-
Summary
-
Risk Management Pitfalls for Smoke Inhalation Injury
-
Time- and Cost-Effective Strategies
-
Case Conclusions
-
Key Points
-
Clinical Pathway for Management of Smoke Inhalation Injury
-
Tables and Figures
-
Table 1. Classification of Inhalation Injury
-
Table 2. History and Physical Examination Findings Suggesting Inhalation Injury
-
Table 3. Carboxyhemoglobin Levels and Associated Symptoms
-
Table 4. RADS Score to Grade Severity of Inhalation Injury on Chest CT
-
Table 5. Abbreviated Injury Score Grading Scale for Inhalation Injury on Bronchoscopy
-
Table 6. Long-Term Complications of Smoke Inhalation Injury
-
Figure 1. Soot and Bronchial Casts From Smoke Inhalation
-
Figure 2. Computed Tomography Scan Slice With Radiologist’s Score Findings
-
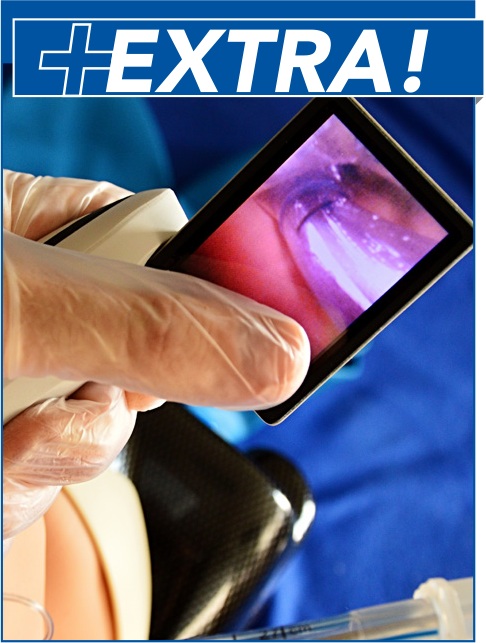
Figure 3. Fiberoptic Laryngoscopy Views of a Normal Airway and an Edematous Airway
-
Figure 4. PaO2/FiO2 Ratio in High-Frequency Percussive Ventilation Compared to Low- Tidal-Volume Ventilation
-
Figure 5. Imaging of Tracheal Wall Thickening on X-Ray, Ultrasound, and Computed Tomography
-
References
Abstract
Smoke inhalation injury portends increased morbidity and mortality in fire-exposed patients. Upper airway thermal burns, inflammation from lower airway irritants, and systemic effects of carbon monoxide and cyanide can contribute to injury. A standardized diagnostic protocol for inhalation injury is lacking, and management remains mostly supportive. Clinicians should maintain a high index of suspicion for concomitant traumatic injuries. Diagnosis is mostly clinical, aided by bronchoscopy and other supplementary tests. Treatment includes airway and respiratory support, lung protective ventilation, 100% oxygen or hyperbaric oxygen therapy for carbon monoxide poisoning, and hydroxocobalamin for cyanide toxicity. Due to its progressive nature, many patients with smoke inhalation injury warrant close monitoring for development of airway compromise.
Case Presentations
A 48-year-old man presents after being rescued from a burning apartment. He complains of shortness of breath and chest tightness. He is coughing up carbonaceous sputum, has soot in his nares, and has 15% total body surface area burns. He is mildly tachypneic, with an oxygen saturation of 92%, and is wheezing. As you continue your primary survey, you wonder what the indications are for intubation in smoke inhalation, and the best approach to this patient’s management...
As you are finishing your evaluation, the patient’s 72-year-old mother is brought in from the same fire. She is obtunded, with 30% total body surface area burns on her torso, extremities, and face. EMS reports that her vital signs are: blood pressure, 100/65 mm Hg; pulse, 105 beats/min; respiratory rate, 16 breaths/min; oxygen saturation, 90% on nonrebreather mask. She does not respond to voice, although she moans and localizes to painful stimuli. As the nurse is checking a fingerstick glucose and placing her on a monitor, you begin your primary survey. You ask your resident to describe the differential diagnosis for altered mental status in a patient with smoke exposure, while in the back of your mind, you begin to weigh the testing and management priorities...
A little later in your shift, a 27-year-old woman who is 18 weeks’ pregnant is triaged for shortness of breath, cough, lightheadedness, mild confusion, and headache. She was in the same apartment complex fire as your previous 2 patients. She cannot recall all the details because she “fainted,” and she regained consciousness only when the firefighters were evaluating her. The EMS crew mentions that the carbon monoxide meter reading in the apartment was elevated. Her vital signs are within normal limits. You suspect carbon monoxide poisoning, but wonder whether she is a candidate for hyperbaric treatment and whether it is safe for the fetus...
Introduction
As these cases highlight, it is not uncommon for multiple patients who have been exposed to a serious fire to present to the emergency department (ED) simultaneously, requiring urgent evaluation and stabilization. Inhalation injuries contribute significantly to morbidity and mortality in fire-exposed patients, and their injuries can range in severity from minimal symptoms to life-threatening injuries. The presence of smoke inhalation injury (SII) is an independent predictor of mortality, and it worsens the prognosis compared to patients of similar age and burned total body surface area (TBSA) without SII.1-3 In patients with cutaneous burns, the presence of a concomitant SII increases fluid requirements, pulmonary complications, and overall mortality.4 Likewise, patients with SII have increased mortality when cutaneous burns are present.5 Data suggest that 5% to 10% of patients hospitalized for burns have a concomitant SII, and that the presence of inhalation injury portends a 20% increased mortality, which increases to 60% higher mortality if secondary pneumonia develops.6 For these reasons, inhalation injury is one of the criteria for transfer to a burn center.7 The diagnosis and prognostication of SII can be challenging due to the lack of standardized severity scoring.1,8 Additionally, it is often difficult to predict severity in the acute phase, since much of the damage is not visible upon initial presentation.9 Various proposed grading schemes have not reliably predicted patient outcomes.6
The insidious nature of SII, both in its delayed development and associated poisoning exposures, cannot be underestimated. The emergency clinician’s ability to suspect, diagnose, and expertly manage SII is crucial. Management is mainly supportive, and some management strategies—such as hyperbaric oxygen, proactive airway management, and ventilation techniques—remain controversial. Standardized diagnostic criteria for SII are lacking, treatment strategies are suboptimal, and morbidity and mortality remain high. This issue of Emergency Medicine Practice presents a comprehensive review of the existing literature, offers best-practice recommendations on the management of patients with SII, and highlights areas where further research is necessary. For information about assessing and treating patients with thermal burns, see the February 2018 issue of Emergency Medicine Practice, “Emergency Department Management of Patients With Thermal Burns,” available at www.ebmedicine.net/Burns.
Selected Abbreviations
|
ALI |
Acute lung injury |
|
ARDS |
Acute respiratory distress syndrome |
|
COHb |
Carboxyhemoglobin |
|
CO |
Carbon monoxide |
|
CN |
Cyanide |
|
FiO2 |
Fraction of inspired oxygen |
|
PaO2 |
Partial pressure of oxygen, arterial |
|
SII |
Smoke inhalation injury |
|
TBSA |
Total body surface area |
Critical Appraisal of the Literature
A literature search was performed via PubMed using the following main search terms: inhalation injury, burns, inhalation, inhalation exposure, smoke inhalation, chemical inhalation, carbon monoxide, carbon monoxide poisoning, hydrogen cyanide, and cyanide. Additional MeSH pairings were used to expand and include airway management strategies, ED patient population, and to limit the studies to those with adult patients and published in English. Once a list of pertinent studies was obtained, we selectively reviewed reference lists to find additional relevant articles. Overall, 1098 articles were identified and 87 were deemed applicable to be included. Many of the identified articles were retrospective studies, case reports, and literature reviews. Some prospective studies exist, but overall, we found a paucity of prospective, blinded, randomized controlled trials pertaining to fire-related inhalation injury.
Risk Management Pitfalls for Smoke Inhalation Injury
3. “The patient had normal vitals and appeared well, so I didn’t anticipate airway compromise.”
The onset of SII can occur in the absence of clinical signs or symptoms, as laryngeal edema can take 24 hours to develop. An extended period of observation is therefore recommended, and if any concerning signs or symptoms of inhalation injury are present, the patient should be admitted to a burn unit for close monitoring and possible bronchoscopy.
6. “When the patient presented with altered mental status, I assumed it was due to hypoxia and chemical toxicity.”
The approach to burn patients should be similar to that of trauma patients, as concomitant traumatic injury is common. Patients should be assessed with a primary survey, followed by a secondary survey. Once the patient is stabilized, occult trauma should be considered in the workup of the patient, especially in the setting of signs such as altered consciousness or pain.
10. “The patient had only mild respiratory distress initially, so I discharged him after 2 hours of observation in the ED.”
Patients should be discharged from the ED only if they are completely asymptomatic, without concerning history for potential SII. Otherwise, if any degree of inhalation injury is suspected, the patient should be transferred to a burn center and admitted for close monitoring and possible bronchoscopic evaluation.
Tables and Figures

References
Evidence-based medicine requires a critical appraisal of the literature based upon study methodology and number of patients. Not all references are equally robust. The findings of a large, prospective, randomized, and blinded trial should carry more weight than a case report.
To help the reader judge the strength of each reference, pertinent information about the study is included in bold type following the reference, where available. In addition, the most informative references cited in this paper, as determined by the authors, are noted by an asterisk (*) next to the number of the reference.
-
* Walker PF, Buehner MF, Wood LA, et al. Diagnosis and management of inhalation injury: an updated review. Crit Care. 2015;19:351. (Review article)
-
Chen MC, Chen MH, Wen BS, et al. The impact of inhalation injury in patients with small and moderate burns. Burns. 2014;40(8):1481-1486. (Retrospective observational study; 21,781 patients)
-
Dokter J, Meijs J, Oen IM, et al. External validation of the revised Baux score for the prediction of mortality in patients with acute burn injury. J Trauma Acute Care Surg. 2014;76(3):840-845. (Prospective cohort study; 4389 patients)
-
Dries DJ, Endorf FW. Inhalation injury: epidemiology, pathology, treatment strategies. Scand J Trauma Resusc Emerg Med. 2013;21:31. (Review article)
-
Mlcak RP, Suman OE, Herndon DN. Respiratory management of inhalation injury. Burns. 2007;33(1):2-13. (Review article)
-
* Sheridan RL. Fire-related inhalation injury. N Engl J Med. 2016;375(5):464-469. (Review article)
-
Cancio LC. Initial assessment and fluid resuscitation of burn patients. Surg Clin North Am. 2014;94(4):741-754. (Review article)
-
Tanizaki S. Assessing inhalation injury in the emergency room. Open Access Emerg Med. 2015;7:31-37. (Review article)
-
Wise B, Levine Z. Inhalation injury. Can Fam Physician. 2015;61(1):47-49. (Review article)
-
Toussaint J, Singer AJ. The evaluation and management of thermal injuries: 2014 update. Clin Exp Emerg Med. 2014;1(1):8-18. (Review article)
-
* Enkhbaatar P, Pruitt BA Jr, Suman O, et al. Pathophysiology, research challenges, and clinical management of smoke inhalation injury. Lancet. 2016;388(10052):1437-1446. (Review article)
-
Antonio AC, Castro PS, Freire LO. Smoke inhalation injury during enclosed-space fires: an update. J Bras Pneumol. 2013;39(3):373-381. (Review article)
-
Toon MH, Maybauer MO, Greenwood JE, et al. Management of acute smoke inhalation injury. Crit Care Resusc. 2010;12(1):53-61. (Review article)
-
Maile R, Jones S, Pan Y, et al. Association between early airway damage-associated molecular patterns and subsequent bacterial infection in patients with inhalational and burn injury. Am J Physiol Lung Cell Mol Physiol. 2015;308(9):L855-L860. (Prospective observational study; 72 patients)
-
Gosling S. Carbon monoxide poisoning: an A&E perspective. Br J Nurs. 1992;1(14):698-704. (Review article)
-
Nikkanen H, Skolnik A. Diagnosis and management of carbon monoxide poisoning in the emergency department. Emerg Med Pract. 2011;13(2):1-14. (Review article)
-
Fortin JL, Giocanti JP, Ruttimann M, et al. Prehospital administration of hydroxocobalamin for smoke inhalation-associated cyanide poisoning: 8 years of experience in the Paris Fire Brigade. Clin Toxicol (Phila). 2006;44 Suppl 1:37-44. (Retrospective chart review; 101 patients)
-
Benner JP, Lawrence D, Brady W. Smoke signals. Recognition and treatment of combustion-induced cyanide toxicity. JEMS. 2009;34(10):56-63. (Review article)
-
Borron SW, Baud FJ, Barriot P, et al. Prospective study of hydroxocobalamin for acute cyanide poisoning in smoke inhalation. Ann Emerg Med. 2007;49(6):794-801, 801.e791-e792. (Prospective study; 69 patients)
-
Lee J, Mukai D, Kreuter K, et al. Potential interference by hydroxocobalamin on cooximetry hemoglobin measurements during cyanide and smoke inhalation treatments. Ann Emerg Med. 2007;49(6):802-805. (Prospective cohort study; 3 rabbits)
-
Pace R, Bon Homme M, Hoffman RS, et al. Effects of hydroxocobalamin on carboxyhemoglobin measured under physiologic and pathologic conditions. Clin Toxicol (Phila). 2014;52(7):647-650. (Comparative experimental model)
-
Livshits Z, Lugassy DM, Shawn LK, et al. Falsely low carboxyhemoglobin level after hydroxocobalamin therapy. N Engl J Med. 2012;367(13):1270-1271. (Case report; 2 cases)
-
Geldner G, Koch EM, Gottwald-Hostalek U, et al. Report on a study of fires with smoke gas development: determination of blood cyanide levels, clinical signs and laboratory values in victims. Anaesthesist. 2013;62(8):609-616. (Prospective interventional study; 102 patients)
-
Pepe G, Castelli M, Nazerian P, et al. Delayed neuropsychological sequelae after carbon monoxide poisoning: predictive risk factors in the emergency department. A retrospective study. Scand J Trauma Resusc Emerg Med. 2011;19:16. (Retrospective chart review; 347 patients)
-
Hampson NB, Hauff NM. Risk factors for short-term mortality from carbon monoxide poisoning treated with hyperbaric oxygen. Crit Care Med. 2008;36(9):2523-2527. (Retrospective chart review; 38 patients)
-
Anseeuw K, Delvau N, Burillo-Putze G, et al. Cyanide poisoning by fire smoke inhalation: a European expert consensus. Eur J Emerg Med. 2013;20(1):2-9. (Review article)
-
Saeui C, Charlton N, Brady WJ. Biochemical issues in emergency medicine: diagnostic and therapeutic considerations of selected toxic presentations. Am J Emerg Med. 2012;30(1):231-235. (Review article)
-
Lawson-Smith P, Jansen EC, Hyldegaard O. Cyanide intoxication as part of smoke inhalation--a review on diagnosis and treatment from the emergency perspective. Scand J Trauma Resusc Emerg Med. 2011;19:14. (Review article)
-
Cancio LC. Airway management and smoke inhalation injury in the burn patient. Clin Plast Surg. 2009;36(4):555-567. (Review article)
-
Ching JA, Ching YH, Shivers SC, et al. An analysis of inhalation injury diagnostic methods and patient outcomes. J Burn Care Res. 2016;37(1):e27-e32. (Database review; 9775 patients)
-
Carrougher GJ. Inhalation injury. AACN Clin Issues Crit Care Nurs. 1993;4(2):367-377. (Review article)
-
Aksu NM, Akkas M, Coskun F, et al. Could vital signs predict carbon monoxide intoxication? J Int Med Res. 2012;40(1):366-370. (Database review; 9775 patients)
-
Hassan Z, Wong JK, Bush J, et al. Assessing the severity of inhalation injuries in adults. Burns. 2010;36(2):212-216. (Retrospective chart review; 105 patients)
-
* Weaver LK. Clinical practice. Carbon monoxide poisoning. N Engl J Med. 2009;360(12):1217-1225. (Review article)
-
Yurtseven S, Arslan A, Eryigit U, et al. Analysis of patients presenting to the emergency department with carbon monoxide intoxication. Turk J Emerg Med. 2015;15(4):159-162. (Retrospective review; 171 patients)
-
Touger M, Birnbaum A, Wang J, et al. Performance of the RAD-57 pulse CO-oximeter compared with standard laboratory carboxyhemoglobin measurement. Ann Emerg Med. 2010;56(4):382-388. (Cross-sectional cohort study; 120 patients)
-
Moon JM, Shin MH, Chun BJ. The value of initial lactate in patients with carbon monoxide intoxication: in the emergency department. Hum Exp Toxicol. 2011;30(8):836-843. (Retrospective cohort study; 102 patients)
-
Inoue S, Saito T, Tsuji T, et al. Lactate as a prognostic factor in carbon monoxide poisoning: a case report. Am J Emerg Med. 2008;26(8):966.e961-e963. (Case report; 1 patient)
-
Icme F, Kozaci N, Ay MO, et al. The relationship between blood lactate, carboxy-hemoglobin and clinical status in CO poisoning. Eur Rev Med Pharmacol Sci. 2014;18(3):393-397. (Prospective study; 201 patients)
-
O’Brien DJ, Walsh DW, Terriff CM, et al. Empiric management of cyanide toxicity associated with smoke inhalation. Prehosp Disaster Med. 2011;26(5):374-382. (Systematic review)
-
Kao HK, Lien TC, Kou YR, et al. Assessment of myocardial injury in the emergency department independently predicts the short-term poor outcome in patients with severe carbon monoxide poisoning receiving mechanical ventilation and hyperbaric oxygen therapy. Pulm Pharmacol Ther. 2009;22(6):473-477. (Retrospective chart review; 81 patients)
-
Yamamura H, Morioka T, Hagawa N, et al. Computed tomographic assessment of airflow obstruction in smoke inhalation injury: relationship with the development of pneumonia and injury severity. Burns. 2015;41(7):1428-1434. (Prospective observational study; 40 patients)
-
Oh JS, Chung KK, Allen A, et al. Admission chest CT complements fiberoptic bronchoscopy in prediction of adverse outcomes in thermally injured patients. J Burn Care Res. 2012;33(4):532-538. (Retrospective study; 44 patients)
-
Koljonen V, Maisniemi K, Virtanen K, et al. Multi-detector computed tomography demonstrates smoke inhalation injury at early stage. Emerg Radiol. 2007;14(2):113-116. (Case report; 1 patient)
-
Garner JP, Jenner J, Parkhouse DA. Prediction of upper airway closure in inhalational injury. Mil Med. 2005;170(8):677-682. (Review article)
-
Albright JM, Davis CS, Bird MD, et al. The acute pulmonary inflammatory response to the graded severity of smoke inhalation injury. Crit Care Med. 2012;40(4):1113-1121. (Prospective observational study; 60 patients)
-
Mosier MJ, Pham TN, Park DR, et al. Predictive value of bronchoscopy in assessing the severity of inhalation injury. J Burn Care Res. 2012;33(1):65-73. (Retrospective review; 32 patients)
-
Endorf FW, Gamelli RL. Inhalation injury, pulmonary perturbations, and fluid resuscitation. J Burn Care Res. 2007;28(1):80-83. (Retrospective chart review; 80 patients)
-
Spano S, Hanna S, Li Z, et al. Does bronchoscopic evaluation of inhalation injury severity predict outcome? J Burn Care Res. 2016;37(1):1-11. (Retrospective review; 160 patients)
-
Palmieri TL. Inhalation injury: research progress and needs. J Burn Care Res. 2007;28(4):549-554. (Review article)
-
Woodson LC. Diagnosis and grading of inhalation injury. J Burn Care Res. 2009;30(1):143-145. (Review article)
-
Kameda T, Fujita M. Point-of-care ultrasound detection of tracheal wall thickening caused by smoke inhalation. Crit Ultrasound J. 2014;6(1):11-11. (Case report; 1 patient)
-
Muehlberger T, Kunar D, Munster A, et al. Efficacy of fiberoptic laryngoscopy in the diagnosis of inhalation injuries. Arch Otolaryngol Head Neck Surg. 1998;124(9):1003-1007. (Prospective cohort study; 11 patients)
-
Cochran A. Inhalation injury and endotracheal intubation. J Burn Care Res. 2009;30(1):190-191. (Review article)
-
McCall JE, Cahill TJ. Respiratory care of the burn patient. J Burn Care Rehabil. 2005;26(3):200-206. (Review article)
-
Dries DJ. Key questions in ventilator management of the burn-injured patient (second of two parts). J Burn Care Res. 2009;30(2):211-220. (Review article)
-
You K, Yang HT, Kym D, et al. Inhalation injury in burn patients: establishing the link between diagnosis and prognosis. Burns. 2014;40(8):1470-1475. (Prospective observation study; 192 patients)
-
Mackie DP. Inhalation injury or mechanical ventilation: which is the true killer in burn patients? Burns. 2013;39(7):1329-1330. (Editorial)
-
Peck MD, Koppelman T. Low-tidal-volume ventilation as a strategy to reduce ventilator-associated injury in ALI and ARDS. J Burn Care Res. 2009;30(1):172-175. (Review article)
-
Dries DJ. Key questions in ventilator management of the burn-injured patient (first of two parts). J Burn Care Res. 2009;30(1):128-138. (Review article)
-
Chung KK, Wolf SE, Renz EM, et al. High-frequency percussive ventilation and low tidal volume ventilation in burns: a randomized controlled trial. Crit Care Med. 2010;38(10):1970-1977. (Randomized control trial; 62 patients)
-
Reper P, Wibaux O, Van Laeke P, et al. High frequency percussive ventilation and conventional ventilation after smoke inhalation: a randomised study. Burns. 2002;28(5):503-508. (Prospective randomized study; 35 patients)
-
Allan PF, Osborn EC, Chung KK, et al. High-frequency percussive ventilation revisited. J Burn Care Res. 2010;31(4):510-520. (Review article)
-
Hall JJ, Hunt JL, Arnoldo BD, et al. Use of high-frequency percussive ventilation in inhalation injuries. J Burn Care Res. 2007;28(3):396-400. (Retrospective review; 122 patients)
-
Hale DF, Cannon JW, Batchinsky AI, et al. Prone positioning improves oxygenation in adult burn patients with severe acute respiratory distress syndrome. J Trauma Acute Care Surg. 2012;72(6):1634-1639. (Prospective study; 18 patients)
-
Carr JA, Phillips BD, Bowling WM. The utility of bronchoscopy after inhalation injury complicated by pneumonia in burn patients: results from the National Burn Repository. J Burn Care Res. 2009;30(6):967-974. (Systematic review; 624 patients)
-
Kallet RH. Adjunct therapies during mechanical ventilation: airway clearance techniques, therapeutic aerosols, and gases. Respir Care. 2013;58(6):1053-1073. (Review article)
-
Sheridan RL, Hess D. Inhaled nitric oxide in inhalation injury. J Burn Care Res. 2009;30(1):162-164. (Review article)
-
Miller AC, Rivero A, Ziad S, et al. Influence of nebulized unfractionated heparin and N-acetylcysteine in acute lung injury after smoke inhalation injury. J Burn Care Res. 2009;30(2):249-256. (Prospective comparative study; 30 patients)
-
Miller AC, Elamin EM, Suffredini AF. Inhaled anticoagulation regimens for the treatment of smoke inhalation-associated acute lung injury: a systematic review. Crit Care Med. 2014;42(2):413-419. (Systematic review; 27 references)
-
Liodaki E, Kalousis K, Schopp BE, et al. Prophylactic antibiotic therapy after inhalation injury. Burns. 2014;40(8):1476-1480. (Retrospective review; 58 patients)
-
Cha SI, Kim CH, Lee JH, et al. Isolated smoke inhalation injuries: acute respiratory dysfunction, clinical outcomes, and short-term evolution of pulmonary functions with the effects of steroids. Burns. 2007;33(2):200-208. (Prospective follow-up study; 96 patients)
-
Weaver LK, Hopkins RO, Chan KJ, et al. Hyperbaric oxygen for acute carbon monoxide poisoning. N Engl J Med. 2002;347(14):1057-1067. (Prospective randomized trial; 228 patients)
-
* Buckley NA, Juurlink DN, Isbister G, et al. Hyperbaric oxygen for carbon monoxide poisoning. Cochrane Database Syst Rev. 2011Apr 13(4):CD002041. (Systematic review; 6 trials, 1361 patients)
-
* Wolf SJ, Maloney GE, Shih RD, et al. Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with acute carbon monoxide poisoning. Ann Emerg Med. 2017;69(1):98-106. (ACEP clinical policy)
-
Huang CC, Ho CH, Chen YC, et al. Hyperbaric oxygen therapy is associated with lower short- and long- term mortality in patients with carbon monoxide poisoning. Chest. 2017;3692(17):30723-7. (Retrospective review; 25,737 patients)
-
Nguyen L, Afshari A, Kahn SA, et al. Utility and outcomes of hydroxocobalamin use in smoke inhalation patients. Burns. 2017;43(1):107-113. (Retrospective chart review; 273 patients)
-
Eckert MJ, Wade TE, Davis KA, et al. Ventilator-associated pneumonia after combined burn and trauma is caused by associated injuries and not the burn wound. J Burn Care Res. 2006;27(4):457-462. (Retrospective chart review; 3388 patients)
-
Belenkiy SM, Buel AR, Cannon JW, et al. Acute respiratory distress syndrome in wartime military burns: application of the Berlin criteria. J Trauma Acute Care Surg. 2014;76(3):821-827. (Retrospective chart review; 201 patients)
-
Roderique EJ, Gebre-Giorgis AA, Stewart DH, et al. Smoke inhalation injury in a pregnant patient: a literature review of the evidence and current best practices in the setting of a classic case. J Burn Care Res. 2012;33(5):624-633. (Literature review)
-
Colohan SM. Predicting prognosis in thermal burns with associated inhalational injury: a systematic review of prognostic factors in adult burn victims. J Burn Care Res. 2010;31(4):529-539. (Systematic review; 13 studies)
-
Edelman DA, White MT, Tyburski JG, et al. Factors affecting prognosis of inhalation injury. J Burn Care Res. 2006;27(6):848-853. (Retrospective chart review; 829 patients)
-
Kadri SS, Miller AC, Hohmann S, et al. Risk factors for in-hospital mortality in smoke inhalation-associated acute lung injury: data from 68 United States hospitals. Chest. 2016;150(6):1260-1268. (Retrospective cohort study; 769 patients)
-
Asmussen S, Maybauer DM, Fraser JF, et al. Extracorporeal membrane oxygenation in burn and smoke inhalation injury. Burns. 2013;39(3):429-435. (Systematic review, meta-analysis; 29 studies)
-
Nosanov LB, McLawhorn MM, Vigiola Cruz M, et al. A national perspective on ECMO utilization in patients with burn injury. J Burn Care Res. 2017;39(2):10-14. (Retrospective review; 30 patients)
-
Held JM, Litt J, Kennedy JD, et al. Surgeon-performed hemodynamic transesophageal echocardiography in the burn intensive care unit. J Burn Care Res. 2016;37(1):e63-e68. (Retrospective observational study; 11 patients)
-
Maybauer MO, Asmussen S, Platts DG, et al. Transesophageal echocardiography in the management of burn patients. Burns. 2014;40(4):630-635. (Systematic review)








 678-366-7933
678-366-7933