 678-366-7933
678-366-7933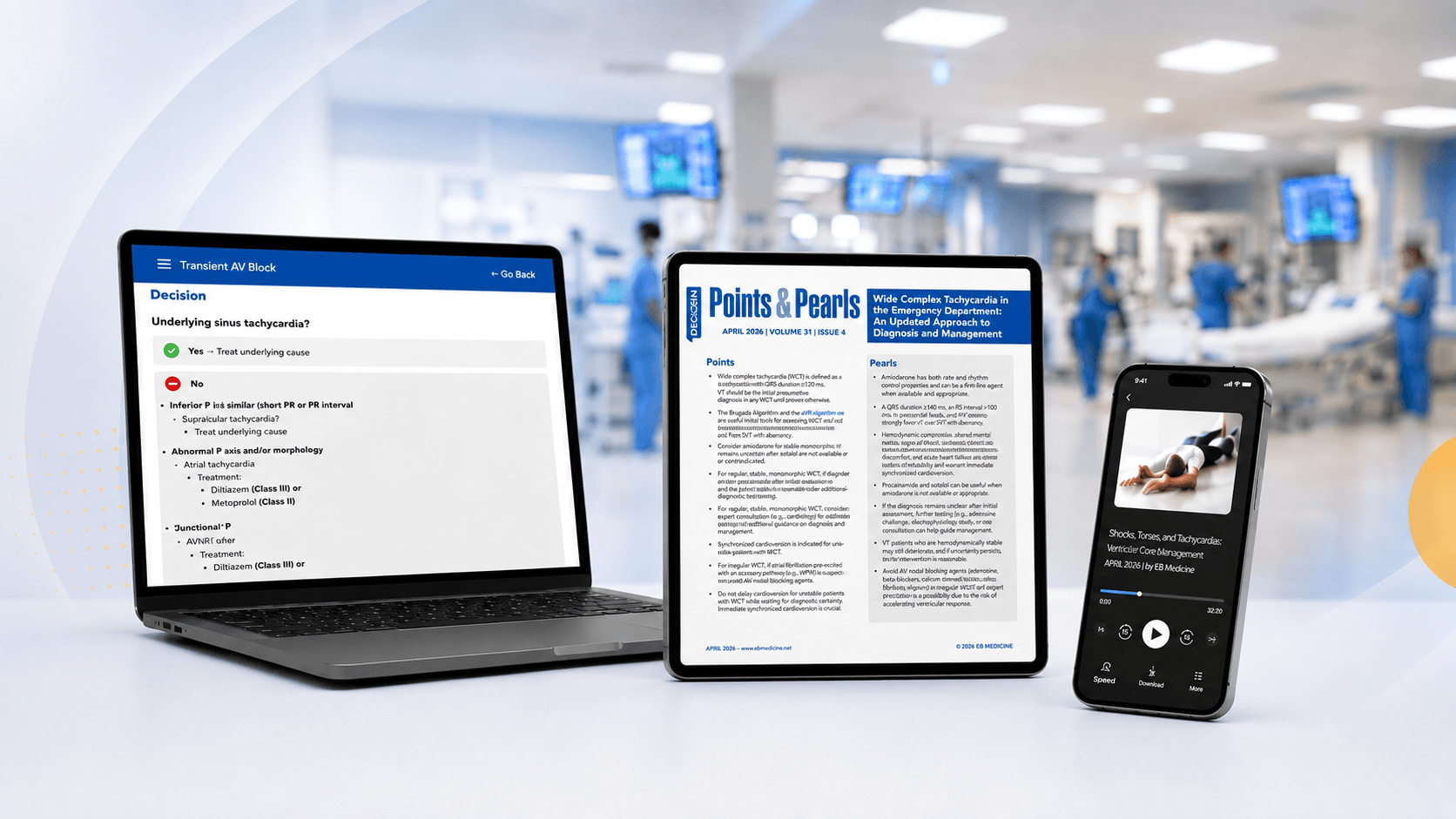











Clinical Skills
The Laceration Course
Master wound repair from simple to complex with step-by-step techniques, documentation, and medico-legal guidance.
On-demand
CME available
Trusted by 33,000+ clinicians · 26 years
Unlimited access to evidence-based journals, clinical pathways, CME, podcasts, and practical tools—all in one subscription.
Trusted by over 33,000 clinicians for 26 years and counting.
Explore Resources Based on Your Discipline or Role.
Earn CME credits with our latest evidence-based emergency medicine and urgent care content.
Emergency Medicine Practice
Pediatric Emergency Medicine Practice
Evidence-Based Urgent Care
Don’t Take Our Word for It. Hear What Others Have to Say About Us.
I subscribe to Emergency Medicine Practice, and Pediatric Emergency Medicine Practice. All of your products are, very simply, the best bang for my CME dollar on any basis of comparison. I'm very impressed!

Gordon L., DO, FACEP, FACOEP
I have been a satisfied subscriber to Emergency Medicine Practice from its inception for several reasons. The main reason was the evidence-based approach the founders took to my discipline's pertinent topics... Customer service has always been superior.
Mike G, MD, MPH, FACEP
I appreciate that you cover topics in-depth, and that you offer a hard copy and audio. I want to hear exactly what the physicians are learning, and you provide that in such a thorough way – that’s why I subscribe!
Rachel Spengler, PA-C
Our success as clinicians is based on how much effort we put into learning. EB Medicine has made that so much easier and has helped me a lot!
Kirsten Miller, MSPAS, PA-C
Short, practical training you can apply on your next shift.
Like you, we recognize the need for excellence in emergency medicine and urgent care and want to have a direct impact on patient care. That's why we are so committed to promoting your clinical education, skills, and best practices, from residency through retirement. Our educational & CME resources help you stay in the know and deliver the highest quality care. If it comes from EB Medicine, you can count on it to be evidence-based, focused, proven in practice, and ready to apply during any future shift.
Accredited By





Our Partners


What is EB Medicine, and who is it for?
EB Medicine provides evidence-based clinical education and CME for emergency medicine, pediatric emergency medicine, and urgent care clinicians.
Since 1999, EB Medicine has created peer-reviewed journals, CME courses, and clinical learning tools that help clinicians stay current, strengthen clinical reasoning, and apply evidence-based recommendations in practice.
EB Medicine publishes:
The “EB” in EB Medicine stands for evidence-based. Our mission is to advance clinical education, skills, and best practices for emergency and urgent care clinicians from residency through retirement.
EB Medicine serves:
EB Medicine content is developed by emergency medicine and urgent care physicians, rigorously peer reviewed, and MEDLINE-indexed by the National Library of Medicine. EB Medicine is also accredited by the Accreditation Council for Continuing Medical Education (ACCME).
Across EB Medicine resources, clinicians have access to 200+ issues and 600+ CME credits.
What do you get with an EB Medicine subscription?
An EB Medicine subscription gives you access to peer-reviewed clinical education, CME credits, searchable issue archives, and practical tools you can use before, during, and after shift in the ED or urgent care.
Depending on your subscription, you can choose:
With a subscription, you receive:
Current subscription libraries include:
Emergency Medicine Practice and Pediatric Emergency Medicine Practice also include EXTRA issues focused on stroke, trauma, and pharmacology.
EB Medicine bundles, like the Emergency Medicine Bundle and Complete Bundle, provide access to multiple subscriptions, allowing you to select the best resources for your practice.
Explore our most popular subscription bundles.
How does EB Medicine help emergency medicine clinicians stay current with best practices?
EB Medicine helps emergency medicine clinicians stay current by turning peer-reviewed evidence into practical, clinically relevant education for the ED.
Each issue includes tools that help translate evidence into action, including decision aids, clinical pathways, risk management pitfalls, tables, and figures across:
More than 10,000 emergency medicine physicians, residents, and advanced practice clinicians subscribe to Emergency Medicine Practice.
In a recent subscriber survey, 99.2% of clinicians said Emergency Medicine Practice improves their quality of patient care.
Learn more about Emergency Medicine Practice.
Learn more about Pediatric Emergency Medicine Practice.
★★★★★ "I have got to tell you—Emergency Medicine Practice is the best-quality emergency medicine learning tool I have seen in my lifetime. In my line of work, I receive and regularly review many sources of information, and this publication is second to none. The effort put into the creation of this publication is evident in every page. Thank you for the tremendous value." — Stephen J. Schueler, MD, FACEP
How does EB Medicine help urgent care clinicians stay current with best practices?
EB Medicine helps urgent care clinicians stay current through Evidence-Based Urgent Care, a monthly, peer-reviewed resource focused on high-yield urgent care presentations.
Each issue breaks down one clinically important topic from presentation to disposition, with clear evidence-based recommendations you can apply in practice, across:
What sets Evidence-Based Urgent Care apart is its focus on clinical reasoning and practical application. You don’t just get the data. You get concise algorithms, interactive clinical pathways, and pitfalls to avoid, so you can understand what to do and why.
The publication is built for urgent care physicians, nurse practitioners, and PAs who want to deepen their clinical confidence through practical, peer-reviewed education or just-in-time learning.
Learn more about Evidence-Based Urgent Care.
★★★★★ "Evidence-Based Urgent Care is a concise but in-depth review of urgent care presentations that can be problematic. It fills a gap for much-needed urgent care education." — John Kulin, DO, FACEP
How much CME is available through EB Medicine?
EB Medicine 600+ CME credits across its full library of subscriptions and courses.
Eligible EB Medicine activities provide AMA PRA Category 1 Credits™. EB Medicine is accredited by the Accreditation Council for Continuing Medical Education (ACCME).
Current subscription CME credits include:
CME credits for courses vary by course.
EB Medicine makes CME reporting easier with:
All issues are designed to meet relevant state and federal CME requirements, including requirements for stroke and trauma centers.
View CME requirements by state.
What topics does EB Medicine cover?
EB Medicine covers evidence-based topics across emergency medicine, pediatric emergency medicine, urgent care, and clinical skills.
You can search EB Medicine by:
Examples of emergency medicine topics include:
Examples of pediatric emergency medicine topics include:
Examples of urgent care topics include:
EB Medicine publishes 36+ new issues and topics each year.
Search available topics.
What courses and clinical skill resources are available through EB Medicine?
EB Medicine offers 10+ clinical courses, with more in development, to help emergency medicine and urgent care clinicians strengthen practical skills.
Course and skills topics include:
Most EB Medicine courses include CME credit, and CME availability varies by course. CME credit for the corticosteroid and antibiotic stewardship courses is not available at this time.
Depending on the course, you may also get practical learning materials such as:
Browse available courses.
★★★★★ "I would recommend The Laceration Course to all new and experienced providers in urgent care and emergency department settings. I think it would also be useful in PA programs as students near the end of clinical year. The course discussed many great suturing pearls that I found to be very helpful." — Gillian Melikian, PA
★★★★★ "I really enjoyed and appreciate attending this excellent EKG course and hope that in the future we could have more of this type of training." — Richard Roman Camps Moreno, MD
What learning formats and tools are included with EB Medicine?
EB Medicine includes multiple learning formats so you can use the content in a way that fits your schedule and workflow.
Available formats include:
EB Medicine also includes practical tools that help you apply evidence to patient care:
These learning formats and practical tools are designed to help you move from evidence to clinical decision-making more efficiently, whether you’re reading a full issue, listening between shifts, reviewing a clinical pathway, completing CME, or practicing a clinical skill.
How are EB Medicine issues created and reviewed?
EB Medicine issues are created through a rigorous editorial process led by experienced physicians, editors, and clinician peer reviewers.
Each issue is built around a clinically relevant topic and developed to help clinicians understand the evidence, recommendations, and reasoning behind patient care decisions.
On average, each EB Medicine issue involves:
The process includes:
EB Medicine’s clinical content is developed and independently peer reviewed by expert practicing clinicians. Generative or AI-assisted tools may not be used to create substantive clinical content, including manuscripts, clinical pathways, recommendations, or clinical interpretations.
AI-enabled tools may be used in a limited way to support research, organization, and production workflows or to create and edit illustrations, graphics, or charts. All AI-assisted materials undergo review and approval by qualified clinician authors and editors before publication.
Read more about EB Medicine’s editorial process.
Can EB Medicine support emergency medicine groups, urgent care teams, hospitals, or residency programs?
Yes. EB Medicine offers group subscription options for hospitals, emergency departments, urgent care groups, and other clinical teams.
Groups can expect a partnership with EB Medicine to provide:
Learn more about a clinical education solution for your emergency medicine or urgent care group.
For residency programs, resident directors can ensure their residents have access to a 100% free resident subscription built to help them build the clinical reasoning skills they’ll rely on throughout their careers.
★★★★★ "I find EB Medicine to be an invaluable and authoritative resource for myself and our hospital. The service we have received has been excellent, and I am very grateful to all of you for that." — Gillian Melikian, PA
How is EB Medicine different from AI-generated answers or general clinical reference resources?
AI tools and general clinical references can help clinicians find information quickly. EB Medicine is different because it’s designed as peer-reviewed clinical education that helps clinicians understand the reasoning behind clinical decisions.
EB Medicine helps you learn:
EB Medicine’s clinical content is developed and independently peer reviewed by expert practicing clinicians.
Generative or AI-assisted tools may not be used to create substantive clinical content, including manuscripts, clinical pathways, recommendations, or clinical interpretations AI-assisted tools may not independently generate clinical images used for diagnosis or clinical decision-making and may not be listed as authors or sources of clinical judgment.
AI-enabled tools may be used in a limited way to support research, organization, production workflows, or the creation and editing of illustrations, graphics, or charts. All AI-assisted materials are reviewed and approved by qualified clinician authors and editors before publication.
EB Medicine isn’t just a quick-answer resource. It’s a CME and clinical education system built to support evidence-based learning, clinical reasoning, and practical application.
Read EB Medicine’s AI policy.
How do I choose the right EB Medicine subscription or resource?
The right EB Medicine resource depends on your role, practice setting, and learning goals.
Choose an EB Medicine bundle like the Emergency Medicine Bundle or Complete Bundle if you want:
Choose Emergency Medicine Practice if you want only emergency medicine clinical education.
Choose Pediatric Emergency Medicine Practice if you want only pediatric emergency medicine clinical education.
Choose Evidence-Based Urgent Care if you want only urgent care clinical education.
Choose from EB Medicine courses if you want focused skill development in areas such as:
Choose resident resources if you want a free emergency medicine clinical subscription during your residency
Choose group access if you’re seeking a clinical education solution for:
How do I get started with EB Medicine?
You can get started with EB Medicine by choosing the subscription, course, or group option that fits your clinical role and needs.
For individual clinicians:
For groups and institutions, tell us more about your needs and goals, and we’ll help you find the right EB Medicine solution for your emergency medicine or urgent care group.
For residents, sign up for a free resident subscription.
Have questions or not sure where to get started? Contact us at 678-366-7933 or ebm@ebmedicine.net.