|
|
Acute monoarticular and polyarticular joint pain can result from infection, trauma, autoimmune, or inflammatory processes. All types may be a major cause of disability that is often preventable with early diagnosis and management. Septic arthritis presents a particular danger, with a high potential for morbidity and mortality. This issue presents an overview of various types of acute joint pain that may present to urgent care, and outlines systematic, evidence-based strategies for diagnosis and treatment. Emerging infectious and reactive causes of arthritis, including Zika, chikungunya, and others are reviewed. Best-practice recommendations for treatment and disposition as well as indications for emergent consultation, emergency evaluation, or specialty referral are also highlighted.
A 27-year-old woman is brought into the urgent care clinic with complaints of severe, diffuse joint pain...
A 72-year-old woman with diabetes and hypertension presents for her third episode of redness and swelling of her right great toe...
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
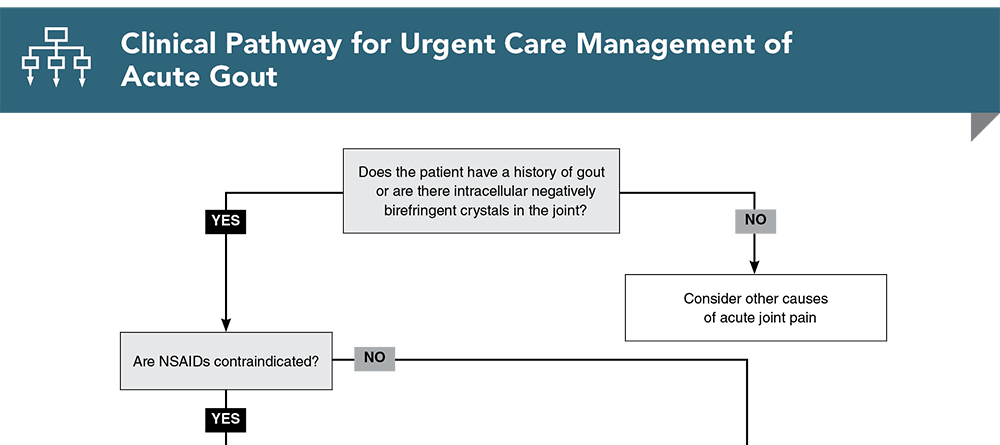
Subscribe to access the complete flowchart to guide your clinical decision making.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
3. * Carpenter CR, Schuur JD, Everett WW, et al. Evidence-based diagnostics: adult septic arthritis. Acad Emerg Med. 2011;18(8):781-796. (Systematic review) DOI: 10.1111/j.1553-2712.2011.01121.x
5. * Long B, Koyfman A, Gottlieb M. Evaluation and management of septic arthritis and its mimics in the emergency department. West J Emerg Med. 2019;20(2):331-341. (Review) DOI: 10.5811/westjem.2018.10.40974
8. Li R, Hatcher J. Gonococcal arthritis. StatPearls [Internet]. Updated May 29, 2023. Accessed November 10, 2023. (Online textbook chapter)
11. US Centers for Disease Control and Prevention. National Notifiable Diseases Surveillance System, 2016 annual tables of infectious disease data. Accessed November 10, 2023. (US government surveillance summary)
30. US Centers for Disease Control and Prevention. Chikungunya virus: diagnostic testing. Updated January 26, 2023. Accessed November 10, 2023. (CDC guidance)
31. US Centers for Disease Control and Prevention. Dengue: areas with risk of dengue. Last reviewed July 12, 2023. Accessed November 10, 2023. (CDC guidance)
32. US Centers for Disease Control and Prevention. Sexually transmitted disease surveillance, 2018. Accessed November 10, 2023. (United States government report)
34. * Margaretten ME, Kohlwes J, Moore D, et al. Does this adult patient have septic arthritis? JAMA. 2007;297(13):1478-1488. (Systematic review; 14 studies, 6242 patients) DOI: 10.1001/jama.297.13.1478
39. * Coakley G, Mathews C, Field M, et al. BSR & BHPR, BOA, RCGP and BSAC guidelines for management of the hot swollen joint in adults. Rheumatology (Oxford). 2006;45(8):1039-1041. (Practice guideline) DOI: 10.1093/rheumatology/kel163a
46. * Punzi L, Oliviero F. Arthrocentesis and synovial fluid analysis in clinical practice: value of sonography in difficult cases. Ann N Y Acad Sci. 2009;1154:152-158. (Review) DOI: 10.1111/j.1749-6632.2009.04389.x
65. United States Centers for Disease Control and Prevention. STI treatment guidelines, 2021: gonococcal infections. Updated September 21, 2022. Accessed November 10, 2023. (CDC guidelines)
66. United States Centers for Disease Control and Prevention. STI treatment guidelines, 2021: managing persons who have a history of penicillin allergy. Updated September 21, 2022. Accessed November 10, 2023. (CDC guidelines)
70. * Terkeltaub RA, Furst DE, Bennett K, et al. High versus low dosing of oral colchicine for early acute gout flare: twenty-four-hour outcome of the first multicenter, randomized, double-blind, placebo-controlled, parallel-group, dose-comparison colchicine study. Arthritis Rheum. 2010;62(4):1060-1068. (Randomized controlled trial; 184 patients) DOI: 10.1002/art.27327
73. * FitzGerald JD, Dalbeth N, Mikuls T, et al. 2020 American College of Rheumatology guideline for the management of gout. Arthritis Care Res (Hoboken). 2020;72(6):744-760. (Practice guidlines) DOI: 10.1002/art.41247
74. * Richette P, Doherty M, Pascual E, et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann Rheum Dis. 2017;76(1):29-42. (Practice recommendations) DOI: 10.1136/annrheumdis-2016-209707
Subscribe to get the full list of 94 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: arthritis, joint, monoarticular, polyarticular, autoimmune, reactive, gout, pseudogout, CPPD, Zika, dengue, Lyme, chikungunya, osteoarthritis, rheumatoid, septic, infectious, gonococcal, crystal, arthrocentesis, synovial, antibiotics
Tracey Quail Davidoff, MD, FCUCM
Amelia Nadler, DNP, FNP-C; Genine Siciliano, MD
December 1, 2023
December 1, 2026 CME Information
4 AMA PRA Category 1 Credits™. 4 AOA Category 2-B Credits. 4 AAFP Prescribed Credits Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 1 Pharmacology and 1 Pain Management CME credit
Evidence-Based Urgent Care • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Evidence-Based Urgent Care issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933