|
|
Traumatic brain injury is a significant cause of long-term disability and death worldwide. Recent advances in the acute management of traumatic brain injury have improved outcomes across the full spectrum of disease, including severe injury. Early recognition, optimization of oxygenation and perfusion, and appropriate disposition are essential components of care for patients with severe traumatic brain injury. A systematic history and physical examination are critical to identifying life-threatening injuries and guiding timely interventions, including management of elevated intracranial pressure. This review summarizes current evidence-based recommendations for the emergency department evaluation and management of severe traumatic brain injury, highlights ongoing controversies, and identifies key areas for future research.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
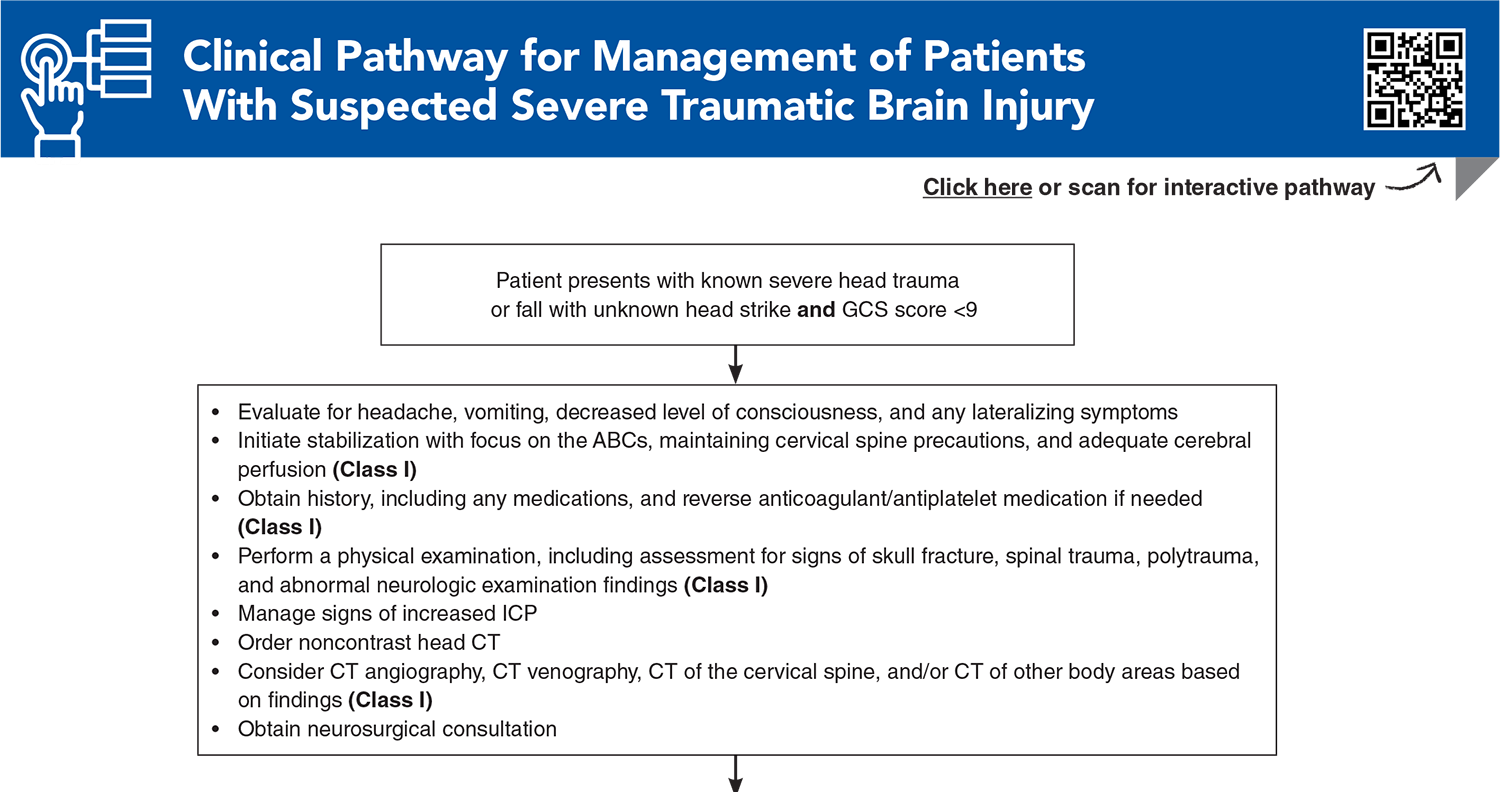
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
5. * Meyfroidt G, Bouzat P, Casaer MP, et al. Management of moderate to severe traumatic brain injury: an update for the intensivist. Intensive Care Med. 2022;48(6):649-666. (Review) DOI: 10.1007/s00134-022-06702-4
8. * Carney N, Totten AM, O'Reilly C, et al. Guidelines for the management of severe traumatic brain injury, fourth edition. Neurosurgery. 2017;80(1):6-15. (Brain Trauma Foundation consensus guidelines) DOI: 10.1227/NEU.0000000000001432
10. * Lulla A, Lumba-Brown A, Totten AM, et al. Prehospital guidelines for the management of traumatic brain injury - 3rd edition. Prehosp Emerg Care. 2023;27(5):507-538. (Brain Trauma Foundation consensus guidelines for prehospital providers) DOI: 10.1080/10903127.2023.2187905
17. * Marehbian J, Muehlschlegel S, Edlow BL, et al. Medical management of the severe traumatic brain injury patient. Neurocrit Care. 2017;27(3):430-446. (Review) DOI: 10.1007/s12028-017-0408-5
25. * Manley GT, Dams-O'Connor K, Alosco ML, et al. A new characterisation of acute traumatic brain injury: the NIH-NINDS TBI classification and nomenclature initiative. Lancet Neurol. 2025;24(6):512-523. (Proposed study framework) DOI: 10.1016/S1474-4422(25)00154-1
35. * Gravesteijn BY, Sewalt CA, Stocchetti N, et al. Prehospital management of traumatic brain injury across europe: a CENTER-TBI study. Prehosp Emerg Care. 2021;25(5):629-643. (Multicenter observational cohort study; 3878 patients) DOI: 10.1080/10903127.2020.1817210
91. * Vrettou CS, Mentzelopoulos SD. Second- and third-tier therapies for severe traumatic brain injury. J Clin Med. 2022;11(16):4790. (Review)
92. * Patel S, Maria-Rios J, Parikh A, et al. Diagnosis and management of elevated intracranial pressure in the emergency department. Int J Emerg Med. 2023;16(1):72. (Review) DOI: 10.1186/s12245-023-00540-x
96. * Muehlschlegel S, Rajajee V, Wartenberg KE, et al. Guidelines for neuroprognostication in critically ill adults with moderate-severe traumatic brain injury. Neurocrit Care. 2024;40(2):448-476. (Clinical practice guideline) DOI: 10.1007/s12028-023-01902-2
97. * Nasrallah F, Bellapart J, Walsham J, et al. PREdiction and Diagnosis using Imaging and Clinical biomarkers Trial in Traumatic Brain Injury (PREDICT-TBI) study protocol: an observational, prospective, multicentre cohort study for the prediction of outcome in moderate-to-severe TBI. BMJ Open. 2023;13(4):e067740. (Observational prospective cohort study protocol) DOI: 10.1136/bmjopen-2022-067740
Subscribe to get the full list of 102 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: TBI, severe, traumatic, intracranial, hemorrhage, pressure, ICP, CPP, EDH, SDH, SAH, herniation, hematoma, intraparenchymal, GCS, midline, CT, MRI, coagulopathy, cerebral perfusion, blood pressure, intubation, hyperosmolar
Dana Klavansky, MD; Anirudha Rathnam, MD, MPH
March 1, 2026
March 1, 2029 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits. Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 4 Trauma CME credits, subject to your state and institutional approval.
Accredited By





Our Partners


 678-366-7933
678-366-7933