

|
|
With almost 2.9 million people in the United States seeking medical attention for head trauma each year, emergency clinicians face the critical task of efficiently and accurately identifying patients with potentially life-threatening intracranial trauma. This issue of Emergency Medicine Practice: Trauma EXTRA! reviews clinical guidelines, discusses challenges in the care of patients at extremes of ages, and provides indications for imaging. Management and disposition of patients with mild traumatic brain injury that includes neurosurgery consultation, hospital admission for observation or repeat imaging, and discharge precautions are also reviewed.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
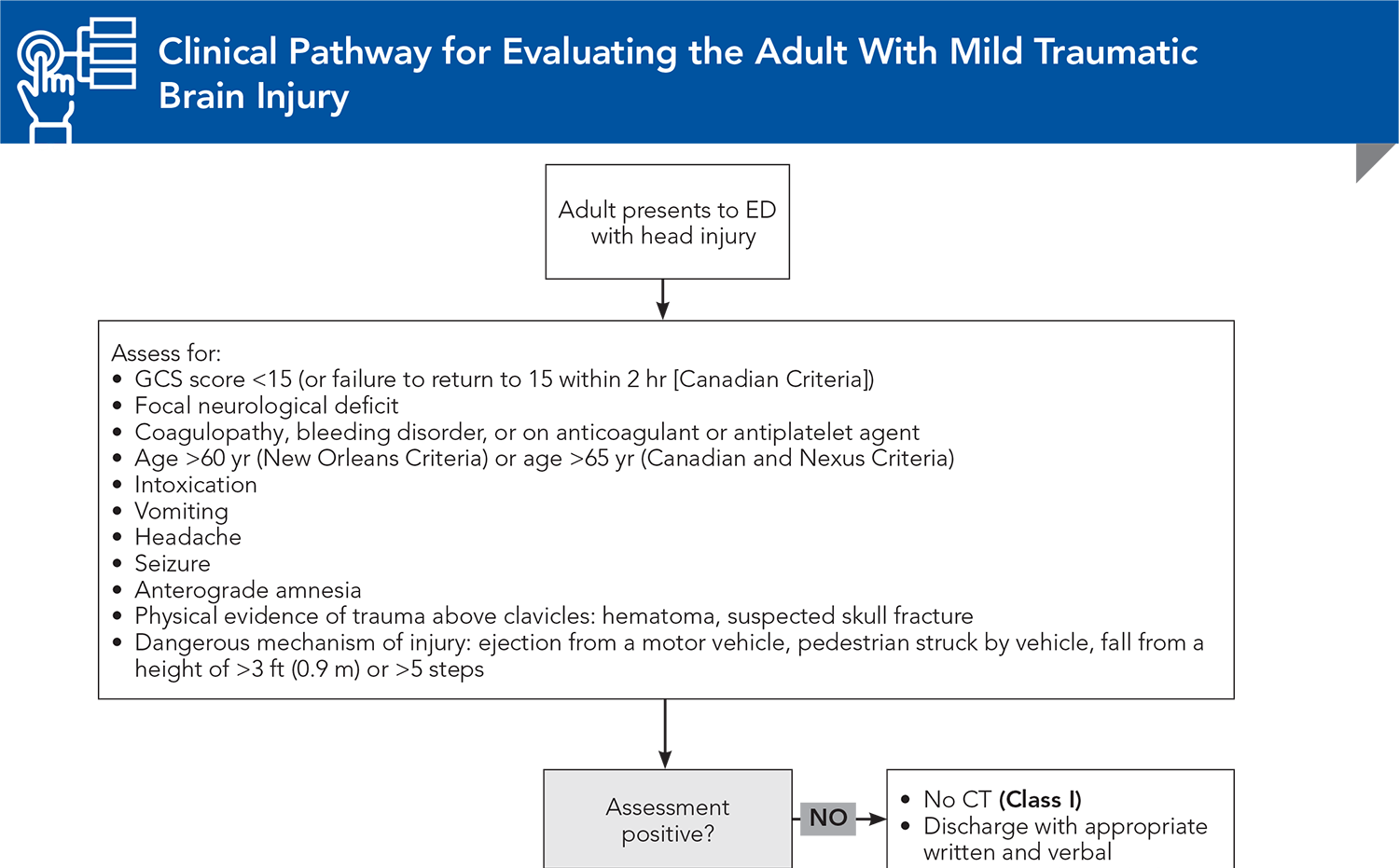
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
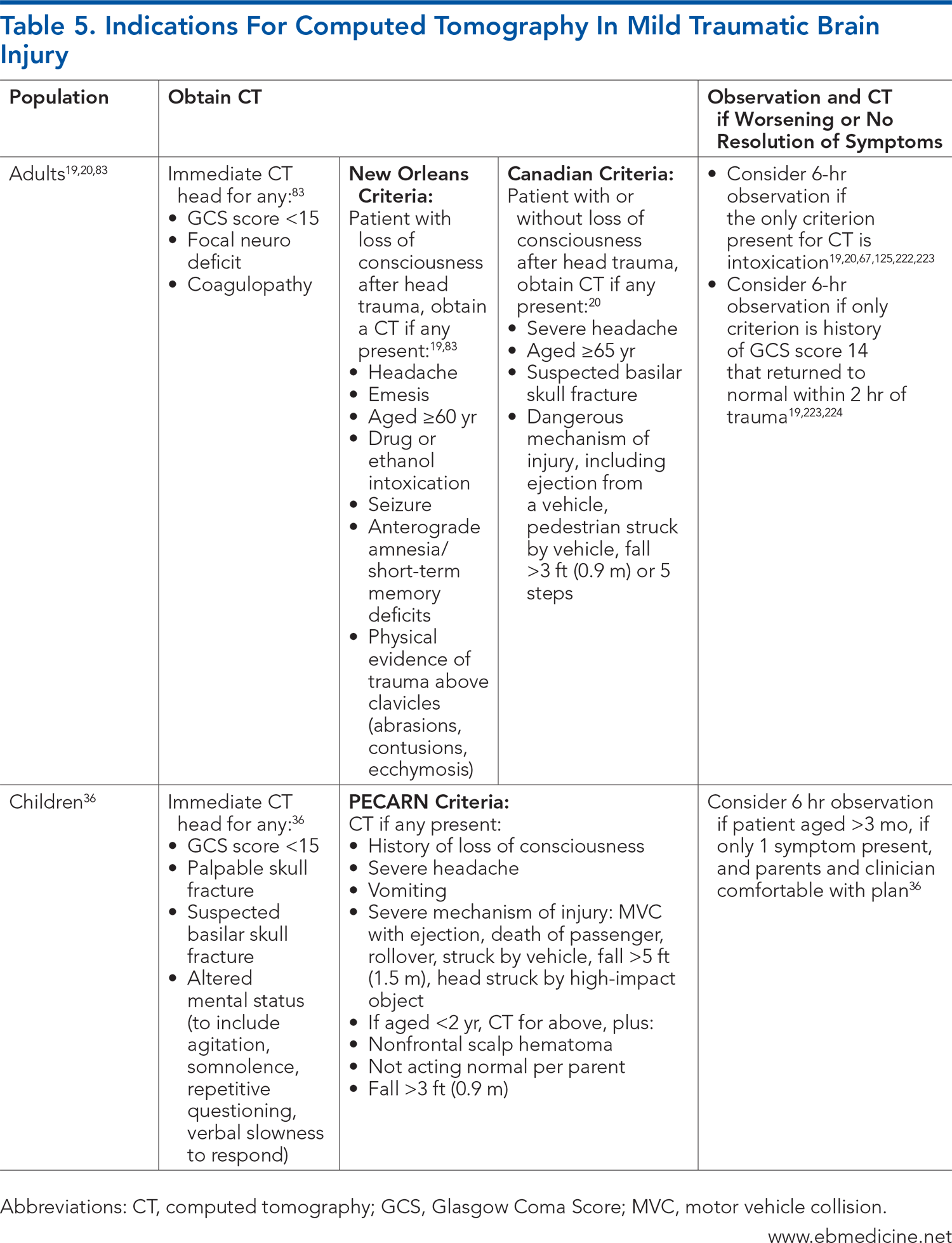
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
12. * Kirelik SB. Concussion in the emergency department: a review of current guidelines. Emerg Med Pract. 2019;21(Suppl 9):1-29. (Guideline review)
13. * Pandor A, Goodacre S, Harnan S, et al. Diagnostic management strategies for adults and children with minor head injury: a systematic review and an economic evaluation. Health Technol Assess. 2011;15(27):1-202. (Systematic review; 93 patients) DOI: 10.3310/hta15270
36. * Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically important brain injuries after head trauma: a prospective cohort study. Lancet. 2009;374(9696):1160-1170. (Prospective study; 42,412 patients) DOI: 10.1016/S0140-6736(09)61558-0
45. * Greenes DS, Schutzman SA. Clinical indicators of intracranial injury in head-injured infants. Pediatrics. 1999;104(4 Pt 1):861-867. (Prospective study; 608 patients) DOI: 10.1542/peds.104.4.861
53. * Nishijima DK, Offerman SR, Ballard DW, et al. Immediate and delayed traumatic intracranial hemorrhage in patients with head trauma and preinjury warfarin or clopidogrel use. Ann Emerg Med. 2012;59(6):460-468.e1-7. (Prospective study; 1064 patients) DOI: 10.1016/j.annemergmed.2012.04.007
94. * Atzema C, Mower WR, Hoffman JR, et al. Defining “clinically unimportant” CT findings in patients with blunt head trauma. Acad Emerg Med. 2002;9(5):451. (Secondary analysis; 8374 patients)
95. * Clement CM, Stiell IG, Schull MJ, et al. Clinical features of head injury patients presenting with a Glasgow Coma Scale score of 15 and who require neurosurgical intervention. Ann Emerg Med. 2006;48(3):245-251. (Secondary analysis; 4551 patients) DOI: 10.1016/j.annemergmed.2006.04.008
96. * Joseph B, Aziz H, Pandit V, et al. Prospective validation of the brain injury guidelines: managing traumatic brain injury without neurosurgical consultation. J Trauma Acute Care Surg. 2014;77(6):984-988. (Guidelines) DOI: 10.1097/TA.0000000000000428
165. * Hamilton M, Mrazik M, Johnson DW. Incidence of delayed intracranial hemorrhage in children after uncomplicated minor head injuries. Pediatrics. 2010;126(1):e33-e39. (Retrospective comparative study; 17,962 patients) DOI: 10.1542/peds.2009-0692
Subscribe to get the full list of 223 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: intracranial injury, concussion, mild traumatic brain injury, intracranial trauma, postconcussive syndrome, head injury, blunt head trauma, cerebral contusions, Glascow Coma Scale, headache, computed tomography, New Orleans Criteria, Canadian CT Head Rule, neurology, Brain Injury Guidelines, sports-related concussion
Micelle Haydel, MD
Tiffany Murano, MD, RDMS, FACEP; Linda Papa, MD.CM, MSc, CCFP, FRCPC, FACEP
February 15, 2025
February 15, 2028 CME Information
4 AMA PRA Category 1 Credits™, 4 AOA Category 2-B Credits. Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 4 Trauma credits, subject to your state and institutional approval.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933