|
|
Motor vehicle collision injuries are frequently seen in urgent care and may be associated with significant patient morbidity and clinician diagnostic uncertainty. Effective evaluation begins with a thorough history and physical examination, with particular attention to the mechanism of injury. In most cases, diagnosis and management are guided by validated clinical decision rules and the judicious use of diagnostic imaging. While many post–motor vehicle collision injuries are minor, urgent care clinicians must be able to identify potentially serious or life-threatening conditions, recognize high-risk populations, and facilitate timely referral to a higher-acuity facility when necessary. This review outlines an evidence-based approach to the evaluation and management of motor vehicle collision-related injuries in the urgent care setting.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
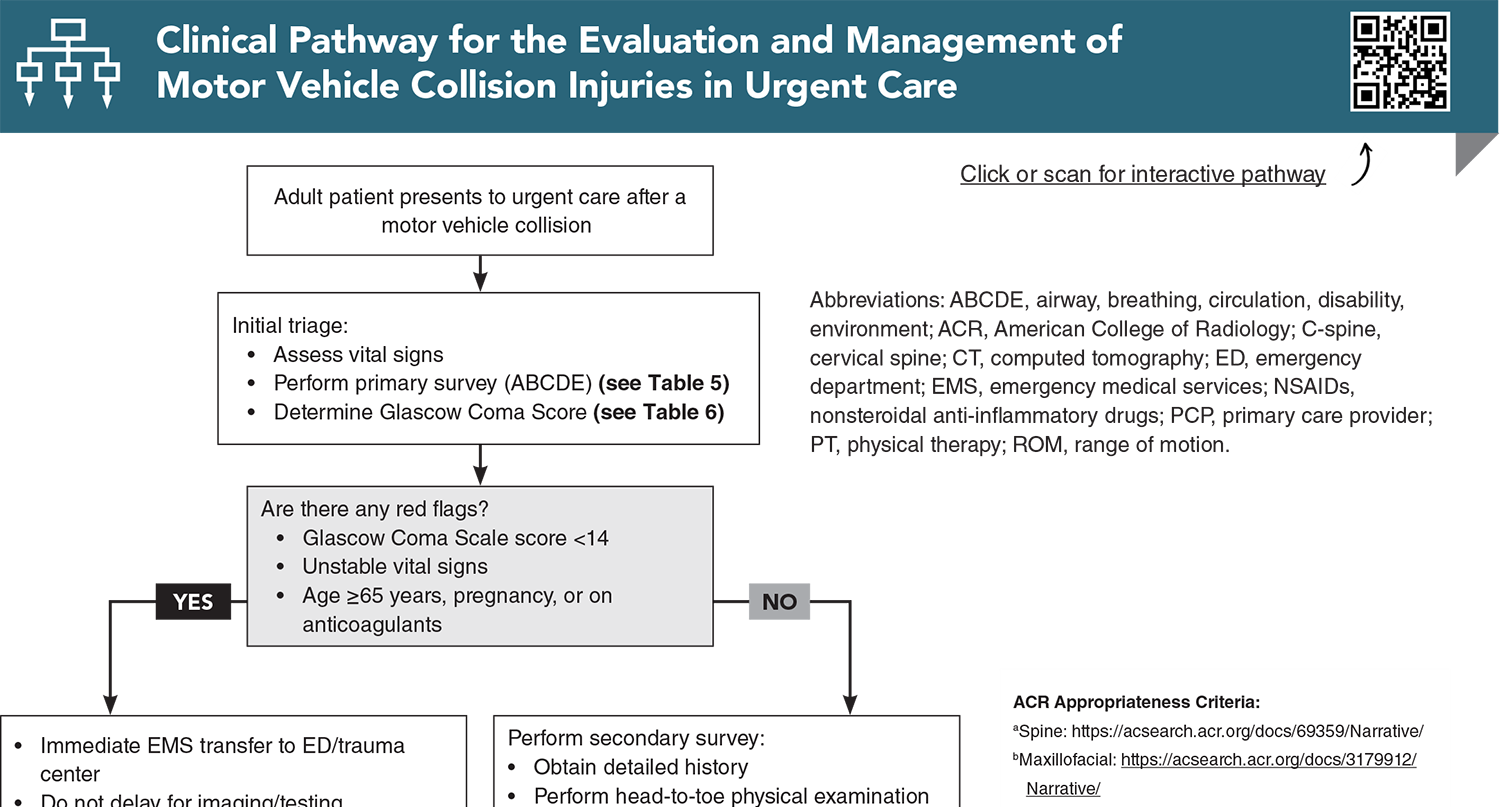
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
7. * Lupton JR, Davis-O’Reilly C, Jungbauer RM, et al. Mechanism of injury and special considerations as predictive of serious injury: a systematic review. Acad Emerg Med. 2022;29(9):1106-1117. (Systematic review) DOI: 10.1111/acem.14489
48. * American College of Emergency Physicians Clinical Policies Subcommittee on Mild Traumatic Brain Injury, Valente JH, Anderson JD, et al. Clinical policy: critical issues in the management of adult patients presenting to the emergency department with mild traumatic brain injury: approved by ACEP board of directors, February 1, 2023 clinical policy endorsed by the Emergency Nurses Association (April 5, 2023). Ann Emerg Med. 2023;81(5):e63-e105. (Review) DOI:
53. * Michaleff ZA, Maher CG, Verhagen AP, et al. Accuracy of the Canadian C-spine rule and NEXUS to screen for clinically important cervical spine injury in patients following blunt trauma: a systematic review. CMAJ. 2012;184(16):E867-E876. (Systematic review; 15 studies) DOI: 10.1503/cmaj.120675
71. * Nishimura E, Finger A, Harris M, et al. One-view chest radiograph for initial management of most ambulatory patients with rib pain. J Am Board Fam Med. 2021;34(1):144-150. (Retrospective cohort study; 1791 patients) DOI: 10.3122/jabfm.2021.01.200276
80. * Velmahos GC, Tatevossian R, Demetriades D. The “seat belt mark” sign: a call for increased vigilance among physicians treating victims of motor vehicle accidents. Am Surg. 2022;65(2):181-185. (Prospective study; 650 patients)
96. * Haj-Mirzaian A, Eng J, Khorasani R, et al. Use of advanced imaging for radiographically occult hip fracture in elderly patients: a systematic review and meta-analysis. Radiology. 2020;296(3):521-531. (Systematic review and meta-analysis; 2992 patients) DOI: 10.1148/radiol.2020192167
Hsu JR, Mir H, Wally MK, et al. Clinical practice guidelines for pain management in acute musculoskeletal injury. J Orthop Trauma. 2019;33(5):e158-e182. (Practice guideline)
116. *Qaseem A, McLean RM, O’Gurek D, et al. Nonpharmacologic and pharmacologic management of acute pain from non-low back, musculoskeletal injuries in adults: a clinical guideline from the American College of Physicians and American Academy of Family Physicians. Ann Intern Med. 2020;173(9):739-748. (Practice guideline) DOI: 10.7326/M19-3602
126. *American College of Surgeons Committee on Trauma. Best practices guidelines in geriatric trauma management. 2023. Accessed December 15, 2025. (Practice guidelines)
Subscribe to get the full list of 147 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: motor vehicle collision, mechanism of injury, Glascow Coma Score, primary survey, secondary survey, Ottawa Knee Rule, Ottawa Ankle Rule, Canadian C-Spine Rule, Canadian CT Head Rule, mild traumatic brain injury, concussion, postconcussive syndrome, moderate traumatic brain injury, Canadian CT Head Rule, central cord syndrome, fracture, Advanced Trauma Life Support (ATLS) Guidelines, ABCDE algorithm, National Emergency X-ray Radiography Utilization Study (NEXUS) Rule, whiplash, whiplash-associated disorder, range of motion, intervertebral disc derangement, central cord syndrome, chest wall injury, chest contusions, pneumothorax, thoracolumbar spine injury, open fracture, crush injury, compartment syndrome, post-traumatic stress disorder, computed tomography, plain radiography, point-of-care ultrasound (POCUS), nonsteroidal anti-inflammatory drugs (NSAIDs)
Frank A. DiFazio, MD, FAAOS; Shelley L. Janssen, MD-MBA
Lisa Campanella-Coppo, MD, FACEP, IFMCP; Kyla Howrish, FNP-C, FCUCM
January 1, 2026 (Reviewed: Dec 2025)
Evidence-Based Urgent Care • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Evidence-Based Urgent Care issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933