

|
|
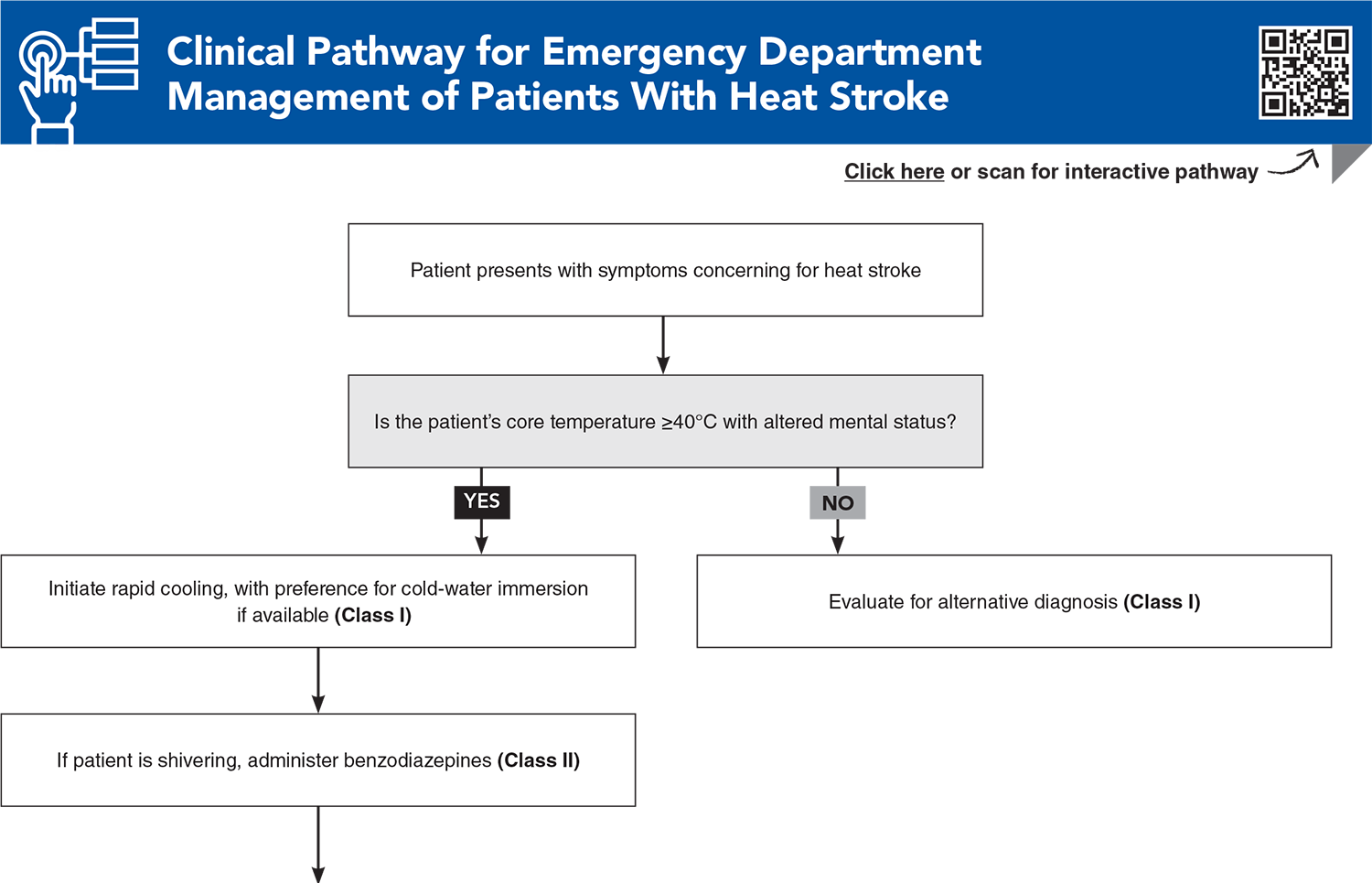
Heat-related illness encompasses a spectrum of conditions ranging from heat cramps and heat exhaustion to life-threatening heat stroke, all resulting from impaired thermoregulation under excessive environmental heat load. The incidence and severity of heat-related illnesses are increasing, underscoring the need for evidence-based emergency management strategies. Accurate diagnosis requires differentiating heat-related illness from conditions that may mimic hyperthermia. Timely recognition and rapid cooling are the cornerstones of management. This review summarizes current evidence on the diagnosis, treatment, and disposition of heat-related illness in the emergency department, with an emphasis on distinguishing heat stroke from conditions with overlapping clinical presentations and on optimizing cooling interventions.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
4. * Kaewput W, Thongprayoon C, Petnak T, et al. Inpatient burden and mortality of heatstroke in the United States. Int J Clin Pract. 2021;75(4):e13837. (Retrospective cohort study; 3372 patients) DOI: 10.1111/ijcp.13837
8. * Barletta JF, Palmieri TL, Toomey SA, et al. Society of Critical Care Medicine guidelines for the treatment of heat stroke. Crit Care Med. 2025;53(2):e490-e500. (Clinical practice guidelines) DOI: 10.1097/CCM.0000000000006551
9. * Eifling KP, Gaudio FG, Dumke C, et al. Wilderness Medical Society clinical practice guidelines for the prevention and treatment of heat illness: 2024 update. Wilderness Environ Med. 2024;35(1_suppl):112s-127s. (Clinical practice guidelines) DOI: 10.1177/10806032241227924
17. * DeGroot DW, Henderson KN, O’Connor FG. Cooling modality effectiveness and mortality associated with prehospital care of exertional heat stroke casualties. J Emerg Med. 2023;64(2):175-180. (Retrospective study; 462 patients) DOI: 10.1016/j.jemermed.2022.12.015
21. * Epstein Y, Yanovich R. Heatstroke. N Engl J Med. 2019; 380(25):2449-2459. (Review) DOI: 10.1056/NEJMra1810762
23. * Belval LN, Casa DJ, Adams WM, et al. Consensus statement- prehospital care of exertional heat stroke. Prehosp Emerg Care. 2018;22(3):392-397. (Expert consensus statement) DOI: 10.1080/10903127.2017.1392666
25. * Rublee C, Dresser C, Giudice C, et al. Evidence-based heatstroke management in the emergency department. West J Emerg Med. 2021;22(2):186-195. (Review) DOI: 10.5811/westjem.2020.11.49007
28. * Roberts WO, Armstrong LE, Sawka MN, et al. ACSM expert consensus statement on exertional heat illness: recognition, management, and return to activity. Curr Sports Med Rep. 2023;22(4):134-149. (Expert consensus statement) DOI: 10.1249/JSR.0000000000000878
43. * Comp G, Pugsley P, Sklar D, et al. Heat stroke management updates: a description of the development of a novel in-emergency department cold-water immersion protocol and guide for implementation. Ann Emerg Med. 2025;85(1):43-52. (Descriptive study and protocol development report) DOI: 10.1016/j.annemergmed.2024.07.013
62. * Hayashida K, Kondo Y, Hifumi T, et al. A novel early risk assessment tool for detecting clinical outcomes in patients with heat-related illness (J-ERATO score): development and validation in independent cohorts in Japan. PLoS One. 2018;13(5):e0197032. (Prospective study; 3001 patients) DOI: 10.1371/journal.pone.0197032
Subscribe to get the full list of 63 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: heat stroke, heat-related illness, heat exhaustion, heat cramps, heat syncope, exertional heat stroke, nonexertional heat stroke, classic heat stroke, hyperthermia, thermoregulation, cold-water immersion, rapid cooling, rhabdomyolysis, neuroleptic malignant syndrome, serotonin syndrome, malignant hyperthermia, thyroid storm, J-ERATO score, heat wave, environmental heat illness, EMS heat protocols
David Fernandez, MD, MHPE; Sophia Gorgens, MD; Carver Goodhue, MD
June 1, 2026
June 1, 2029 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933
