

|
|
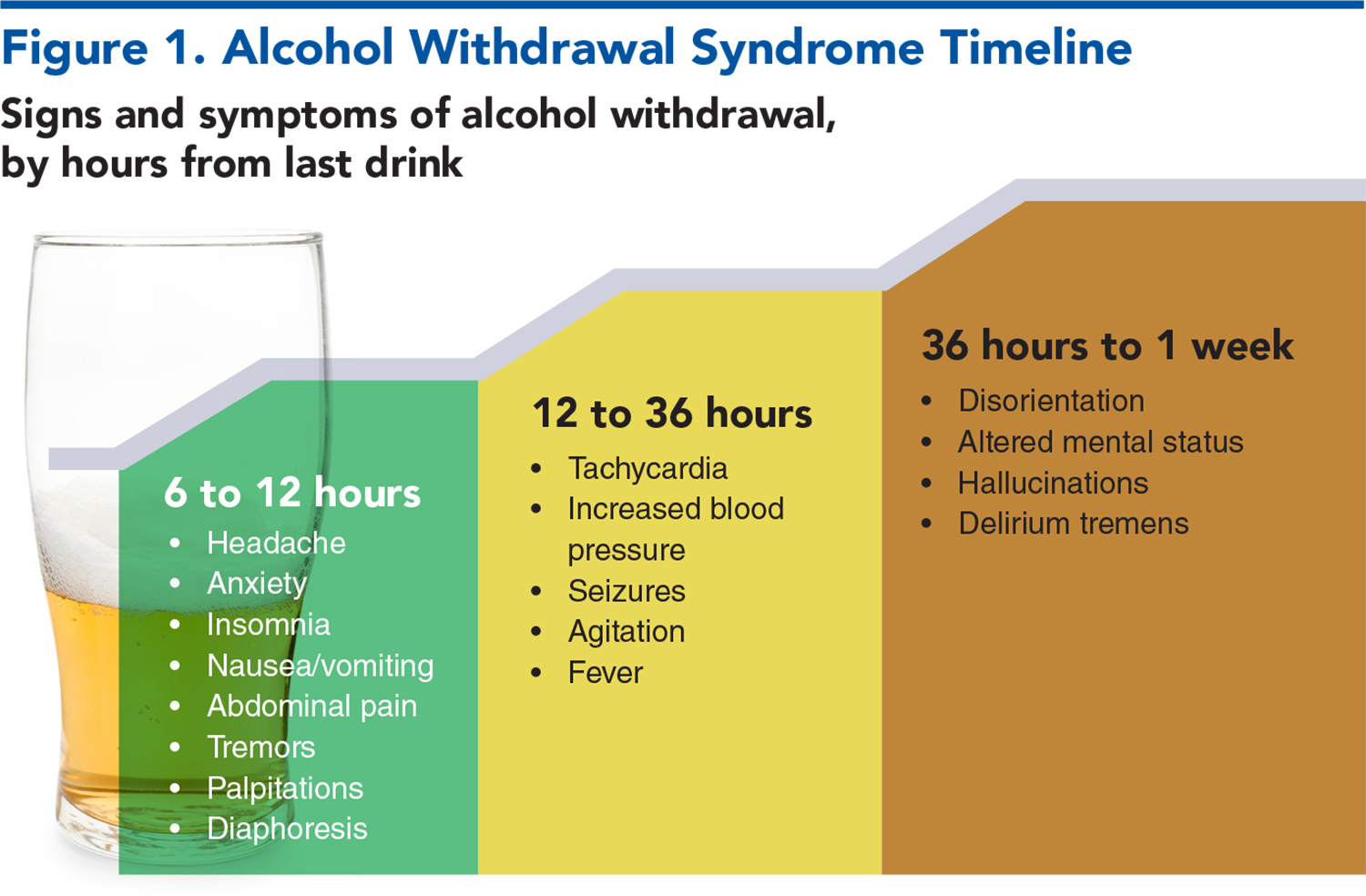
Alcohol withdrawal syndrome is a constellation of symptoms and signs resulting from the abrupt decrease or cessation of heavy alcohol use. Complications of alcohol withdrawal syndrome present significant dangers for patient morbidity and mortality, as well as burdens on emergency department resources. This review presents an overview of the pathophysiology of alcohol withdrawal syndrome and a systematic approach for management in the emergency department. Current evidence on treatment regimens and adjunctive therapies is reviewed, and recommendations for management of patients with alcohol use disorders are discussed.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
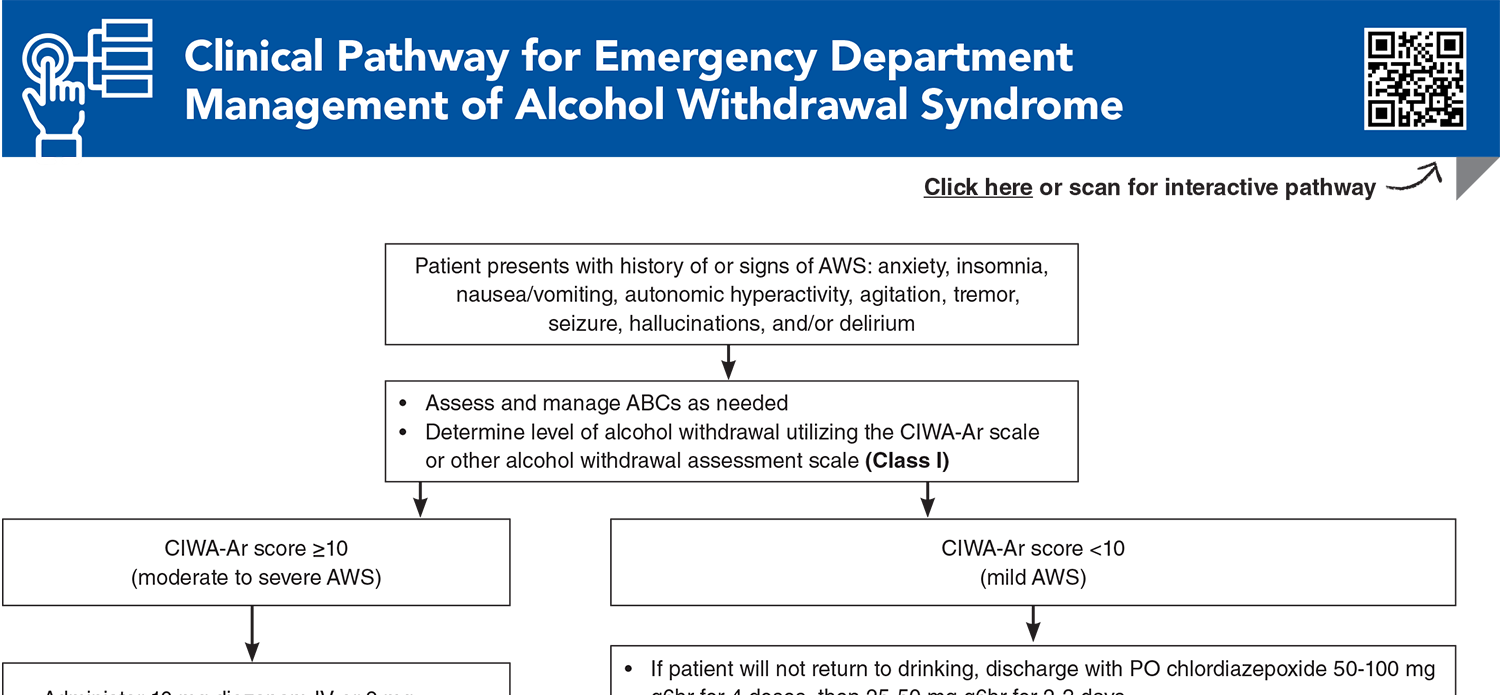
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
1. * Strayer RJ, Friedman BW, Haroz R, et al. Emergency department management of patients with alcohol intoxication, alcohol withdrawal, and alcohol use disorder: a white paper prepared for the American Academy of Emergency Medicine. J Emerg Med. 2023;64(4):517-540. (White paper/clinical guidelines) DOI: 10.1016/j.jemermed.2023.01.010
4. * Kast KA, Sidelnik SA, Nejad SH, et al. Management of alcohol withdrawal syndromes in general hospital settings. BMJ. 2025;388:e080461. (Review) DOI: 10.1136/bmj-2024-080461
7. * The ASAM clinical practice guideline on alcohol withdrawal management. J Addict Med. 2020;14(3S Suppl 1):1-72. (Clinical practice guidelines) DOI: 10.1097/ADM.0000000000000668
8. * Borgundvaag B, Bellolio F, Miles I, et al. Guidelines for reasonable and appropriate care in the emergency department (GRACE-4): alcohol use disorder and cannabinoid hyperemesis syndrome management in the emergency department. Acad Emerg Med. 2024;31(5):425-455. (Clinical practice guidelines) DOI: 10.1111/acem.14911
71. * Pourmand A, AlRemeithi R, Kartiko S, et al. Evaluation of phenobarbital based approach in treating patient with alcohol withdrawal syndrome: a systematic review and meta-analysis. Am J Emerg Med. 2023;69:65-75. (Systematic review and meta-analysis; 12 articles, 1934 patients) DOI: 10.1016/j.ajem.2023.04.002
85. * Wolf C, Curry A, Nacht J, et al. Management of alcohol withdrawal in the emergency department: current perspectives. Open Access Emerg Med. 2020;12:53-65. (Review) DOI: 10.2147/OAEM.S235288
106. *McPheeters M, O’Connor EA, Riley S, et al. Pharmacotherapy for alcohol use disorder: a systematic review and meta-analysis. JAMA. 2023;330(17):1653-1665. (Systematic review and meta-analysis; 118 articles; 20,976 patients) DOI: 10.1001/jama.2023.19761
Subscribe to get the full list of 123 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: ethanol, tachycardia, withdrawal, hypertension, tremor, diaphoresis, benzodiazepine, CIWA-Ar, hallucinosis, seizure, delirium, kindling, phenobarbital, ketamine, gabapentin, anti-craving
Alex Y. Koo, MD, FACEP, FAAEM
Christopher Hahn, MD; Reuben J. Strayer, MD, FACEP, FASAM
November 1, 2025
November 1, 2028 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits. Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 4 Substance Use Disorders CME credits and 4 Pharmacology CME credits, subject to your state and institutional approval.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933


