
Perhaps no other sensation can evoke such fear as the inability to breathe. Dyspnea rivals sensations like hunger or thirst.1 There are numerous causes for dyspnea that range from the benign to life-threatening, and the emergency physician must quickly distinguish the innocuous from the grave. The question is, at what cost? Which patients need only reassurance, and which require an extensive (and expensive) diagnostic work-up?
Patient anxiety may be a major source of diagnostic confusion. A diagnosis of anxiety provides a simple explanation for many cases of dyspnea seen in the ED. But while anxiety can produce breathlessness, lifethreatening diseases also generate hyperventilation in patients and physicians alike. This issue of Emergency Medicine Practice will decrease your trepidation in dealing with this common complaint.
Dyspnea is the perception of the inability to breathe comfortably.2 Although dyspnea is subjective, it has a physiologic basis. Chemoreceptors and stretch receptors interact with the brain and lungs to modulate respirations. Of note, respirations are the only vital sign subject to voluntary control.
Chemoreceptors detect changes in blood oxygen and carbon dioxide and subsequently trigger the respiratory drive centers. Decreased ventilation and increased lung deadspace both elevate PCO2. Lung deadspace expands when lung units are ventilated but not perfused, such as in pulmonary embolism. While elevations in CO2 are a crucial stimulant of respiratory drive, this mechanism is often blunted in patients with chronic lung disease. Other chemoreceptors are responsible for detection of acidosis, which will also increase respiratory drive.
Hypoxemia also modulates respirations through chemoreceptors. When the carotid body senses a minute fall in oxygen tension, it stimulates the brainstem to increase ventilation. The most common cause of hypoxemia is pulmonary ventilation-perfusion mismatch. This imbalance between pulmonary blood flow and alveolar ventilation is usually due to diseases of the heart or lung. Shunt is an extreme form of ventilation-perfusion mismatch and occurs when ventilation to a lung unit is interrupted despite persistent blood flow.3,4 Thus, the blood shunts past this "dummy" area of lung without exchanging gases. During shunt, the body compensates with reflex pulmonary vasoconstriction, which attenuates blood flow to non-ventilated lung units. While b2-adrenergic agents can reverse this vascular response, supplemental oxygen cannot correct hypoxemia produced by shunt.
Heightened airway resistance, elevated lung deadspace, and abnormal lung stiffness all increase the work of breathing.3,5,6 Mechanoreceptors in the face, upper airway, chest wall, and lungs are responsible for a feedback loop that modulates this sensation; vagal J receptors in the lung are important mediators.5 Researchers believe that the mismatch between lung volume and tension in the muscles of respiration is another important factor in patients with increased work of breathing.1
Even "psychogenic" dyspnea has a physiologic basis. Changes in brain neurochemistry and unusual responsiveness to PCO2 may be responsible for the breathlessness of panic disorders.7

In three prospective studies, 207 patients underwent comprehensive laboratory and physiological testing for chronic dyspnea. A cardiac or pulmonary problem was the primary etiology in three-quarters of the cases.10-12 In these settings, most cases of dyspnea were due to one of the following processes: hyperactive airways or chronic obstructive pulmonary disease (COPD), congestive heart failure (CHF), acute pneumonia, or acute pulmonary embolism (PE).
Although it is difficult to track the prevalence of isolated dyspnea in adult ED, approximately 2-3% of all ED patients complain of respiratory distress.13,14
Many patients have dyspnea in conjunction with another symptom, such as diaphoresis, chest pain, palpitations, cough, or fever. These associated symptoms may provide important clues to the etiology.
An important goal in emergency medicine is detection of serious or life-threatening causes of dyspnea. For this reason, psychogenic dyspnea should be diagnosed after exclusion of organic causes. This does not require extensive diagnostic testing in all cases. History, physical, and simple ED tests may obviate the need for further studies. Patients previously in good health with dyspnea who are younger than 40 are diagnosed with psychogenic dyspnea in one-third of ED visits.10
Another important goal is detection of PE. Pulmonary embolism is of special import, not just because of potential lethality, but because patients may not appear critically ill. While there are other serious causes of dyspnea, such as pulmonary edema, profound acidosis, and pericardial tamponade, these patients appear supremely distressed. They present with dramatic findings on examination and are unlikely to be discharged by even the unwary clinician. On the other hand, the patient with pulmonary embolism may exhibit only modest findings, inviting a superficial evaluation.
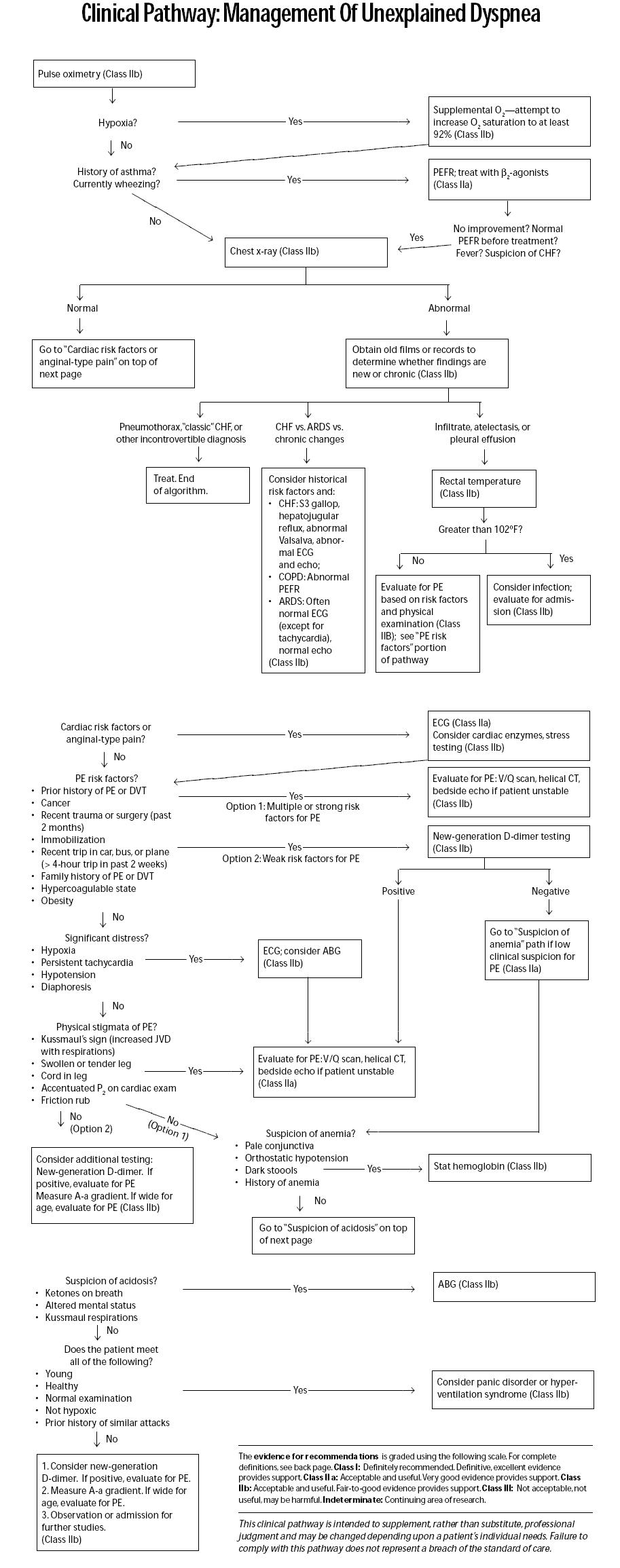
The history, physical examination, and chest film will accurately predict the cause of dyspnea in about twothirds of patients.11These three basic investigations will frequently determine the need for other studies. The Clinical Pathway "Management Of Unexplained Dyspnea" summarizes the approach to patients with dyspnea.
History will provide important clues to the diagnosis and the need for further investigation. Determine the patient's risk for serious disease. Of particular importance is the patient's age, past medical conditions, and associated symptoms.
Was the onset immediate or gradual, and is the dyspnea acute, chronic, or recurring? The duration of symptoms before presentation provides important information. Patients with symptoms for longer than two weeks are more likely to have mild congestive failure, anemia, pulmonary hypertension, chronic lung disease, or recurrent pulmonary embolism.
The events surrounding acute dyspnea may be revealing. Was the patient eating (suggesting the presence of a foreign body or allergic reaction)? Was the patient SCUBA diving (suggesting that the patient has an air embolism or pneumothorax)?
The language a patient uses to describe dyspnea varies with age, ethnicity, and severity of the underlying etiology.2,15 Patients may use terms such as "shortness of breath," "shortness of wind," "breathlessness," "trouble breathing," "suffocating," "chest tightness," "breathing at the top of my lungs," or "heavy breathing." Normal volunteers who are subjected to various experimental causes of dyspnea (ranging from low oxygen to increased work of breathing) can distinguish the cause of dyspnea through their choice of descriptors.2 Patients with the same diagnoses tend to use similar language to describe their symptoms.15 Thus, it is possible that the patient's words can help to target his or her particular pathophysiology.(See Table 2 for some examples.)

Ask patients to grade the severity of the dyspnea. The modified Borg scale is employed by many pulmonary clinics. (See Table 3.) Like the numerical scale used to grade the severity of chest pain, the Borg scale measures the severity of dyspnea from 0 to 10. Zero represents no shortness of breath, while a 10 signifies severe, oppressive symptoms. Simon et al showed that acute asthma, COPD, and CHF all produce severe dyspnea (7 out of 10), whereas dyspnea associated with normal pregnancy, neuromuscular causes, or PE was described as moderate by most patients (5 out of 10).15 (Note that a potentially lethal cause of dyspnea caused only moderate shortness of breath!)

The associated symptoms provide focus to the emergency evaluation, and the presence of chest pain is of special concern.15The location and quality of the pain may help narrow the differential diagnosis. Cardiac pain tends to be more substernal and constant, while the pain of pneumonia and pulmonary embolism is usually more peripheral and tends to increase with respirations. Interestingly, in the PIOPED (Prospective Investigation of Pulmonary Embolism Diagnosis) study, no patient with PE had radiation of pain to the arms.16
Cough is nonspecific and may represent asthma, pneumonia, PE, heart failure, or bronchitis. Fever is also nonspecific and may occur with infection or PE. However, patients with PE rarely have a fever greater than 102°F.16 While dyspnea with exertion often suggests congestive failure, it may occur with reactive airway disease, PE, pneumonia, anemia, or physical deconditioning. Orthopnea occurs with both cardiac and pulmonary causes of dyspnea.
Past medical history is often illuminating. Ask the patient, "Has this ever happened to you before?" The patient who mutely responds with an empty canister of albuterol makes an eloquent statement. Always ask regarding a prior history of PE or deep venous thrombosis (DVT). A prior history of thromboembolic disease may mandate extensive testing for PE. Some patients, however, mistake a prior evaluation for PE to represent a diagnosis of PE. Others believe having a varicose vein or a hematoma on the leg represents a "blood clot." If patients report prior PE or DVT, determine whether they were
ever on warfarin.
Ascertain whether the patient has taken a new drug or is compliant with chronic medications. A new prescription for beta-blockers or calcium-channel blockers can precipitate congestive heart failure, while aspirin abuse may cause metabolic acidosis. The use of birth control pills or other estrogen products increases the risk of PE in women who smoke.
The social history is rarely emphasized in emergency practice; however, this aspect of the interview is important in the patient with dyspnea. For instance, a patient who does not smoke cigarettes is very unlikely to have COPD.11 HIV risk factors become important in the patient with possible pneumonia.
The astute emergency physician can identify the patient in respiratory distress from across the room. Unless moribund, the patient is anxious and is usually sitting bolt upright, employing the neck and chest muscles to assist in ventilation. He or she may be unable to speak or only capable of gasping short phrases. The skin is often dusky and diaphoretic. Fortunately, few patients present with such drama. However, with attention to various aspects of the physical examination, the emergency physician can frequently detect the cause of dyspnea.
Vital signs are crucial in the evaluation of the dyspneic patient. Hypotension and dyspnea are an ominous combination that may be due to a variety of etiologies…all bad. Eight percent of patients with PE may present in shock.16 Other considerations include cardiac etiologies, tension pneumothorax, occult hemorrhage, and metabolic disorders.
In patients with possible heart failure, consider measuring the proportional pulse pressure. The proportional pulse pressure is calculated using the following formula: (systolic pressure - diastolic pressure)/systolic pressure. A ratio of less than 0.25 predicts left ventricular systolic dysfunction.17
Tachycardia is generally a nonspecific finding, but persistent tachycardia requires explanation and often
further testing.
Measurement of the respiratory rate deserves care. A normal respiratory rate ranges from 15-24 breaths per minute in the healthy adult. Patients on the lower end of normal are unlikely to have PE, as fewer than 15% of patients with PE have respiratory rates less than 20 breaths per minute.16,18 When measuring the respiratory rate, evaluate the patient during at least 30 seconds of quiet observation. In the histrionic patient, respirations counted surreptitiously from outside the room may be helpful.
Look in the mouth of patients with unexplained dyspnea. The presence of oral thrush will quickly narrow the differential diagnosis. Dyspnea on exertion is a common complaint of patients with Pneumocystis carinii pneumonia (PCP).
Evaluation of the neck veins can also be useful. Jugular venous distention is seen with right heart failure. Kussmaul's sign, a paradoxical increase in the neck veins with inspiration, occurs with pericardial tamponade, PE, pneumothorax, and right ventricular infarction.
Stridor, as opposed to wheezing, is likely to represent upper airway obstruction.
General. Evaluate the duration of the inspiratory and expiratory phases of respiration. A prolonged expiratory phase (greater than twice the inspiratory phase) suggests obstructive lung disease. Listen to this patient's speech. Does he or she need to stop during each sentence to gasp for air?
Inspection. Look for the previously mentioned signs of respiratory distress, such as intercostal retractions, accessory muscle use, and nasal flaring. Patients with airway obstruction may demonstrate paradoxical sternal retractions with inspiration, a finding more prominent in children.
Palpation. Palpation is rarely helpful in the absence of trauma. However, a patient with spontaneous pneumothorax may occasionally have subcutaneous air palpable at the root of the neck.
Percussion. Traditionally, percussion is used to detect effusions, infiltrates, and pneumothorax. The traditional technique of tapping with a finger or hammer on the chest is employed with spotty frequency and success in the ED. However, a variation of this technique, termed the "auscultatory-percussion" test, is both useful and generally unknown to the emergency physician.
To perform this test, tap on the second thoracic vertebra and use a stethoscope to compare the percussion notes on each side of the anterior and lateral chest. Then tap on the sternum while listening to each side of the posterior chest. If the percussion note on one side is different in intensity or character from its "mirror image" sound on the other, the test is positive, and the patient is likely to have an abnormality on chest radiography. Some studies suggest that this test is more sensitive than simple auscultation for a variety of pulmonary diseases.19,20 Other studies have not shown such positive results.
Auscultation. This aspect of the physical examination will likely direct further management. A unilateral decrease in breath sounds should raise consideration for a spontaneous pneumothorax, atelectasis, pleural effusion, or pneumonia.
Auscultate the lungs for wheezing and rales. While these are signs of pathology, they are very nonspecific. All that wheezes is not asthma; wheezing may occur with foreign bodies, pneumonia, congestive heart failure, or PE. Rales may occur with pneumonia, interstitial lung disease, COPD, or CHF. In CHF, rales are neither sensitive (13%) nor specific predictors of systolic dysfunction. However, the absence of rales eliminates 98% of patients with interstitial lung disease.11 Rales are common in PE, and one-half of such patients with angiographically confirmed PE may demonstrate rales on physical exams.18
Some believe that the traditional chest physical examination alone is not sufficiently accurate to confirm
or exclude the diagnosis of pneumonia. In one study, the most valuable examination maneuvers in detecting pneumonia were unilateral rales and rales in the lateral decubitus position.21
Auscultate the heart. An S3 gallop is a significant finding that suggests congestive heart failure. Murmurs may also be revealing. Important murmurs include the diastolic murmur (and opening snap) of mitral valve stenosis and the systolic murmur of aortic stenosis. Rupture of a papillary muscle may result in acute mitral regurgitation and a loud systolic murmur radiating to the axilla. An accentuated component of the second heart sound may occur in more than half of the patients with angiographically proven PE.18 (Although it would be an impressive clinician indeed who could make this diagnosis simply upon listening to the heart!)
Examine the extremities for evidence of cyanosis and edema. While peripheral edema is common in patients with right-sided or biventricular failure, it is usually absent in patients with acute left ventricular dysfunction. Look for stigmata of chronic hypoxia such as clubbing. Dyspneic patients with unilateral leg swelling, calf tenderness, or distended superficial veins are likely to have PE.22 However, most patients with PE do not have any extremity signs or symptoms.
The skin exam is normal in most patients with dyspnea. Cyanosis is rare and may be caused by either severe methemoglobinemia or profound hypoxemia. The anemic patient may not be cyanotic despite severe hypoxemia, as this requires at least 5 grams of unsaturated hemoglobin. 23 Diaphoresis denotes sympathetic overdrive and is common with CHF and ischemic disease. Its presence in an asthmatic patient is worrisome.
There are two diagnostic maneuvers that are useful in patients who complain of shortness of breath; both target the individual at risk for cardiac dysfunction. The simplest maneuver is hepatojugular reflux. In patients with heart failure, pressing on the liver should result in distention of the neck veins.24
The second test involves a maneuver similar to that used in measuring the pulsus paradoxus.25 The patient must grunt (Valsalva) while a blood pressure cuff is inflated 15 mmHg above their systolic pressure. In a patient with normal cardiac function, the physician will hear the patient's heartbeat immediately after release of the cuff. In the presence of systolic dysfunction, return of the auscultated heartbeat is delayed after cuff deflation, or else it persists throughout cuff inflation and deflation.
The most useful diagnostic tests in the evaluation of dyspnea are simple, widely available, and relatively
inexpensive. These are the pulse oximetry and the chest x-ray.
Some consider oxygen saturation as the "fifth vital sign," and its role in emergency medicine seems boundless. In some large EDs, all patients who present to triage receive a screening pulse oximetry.
Pulse oximetry is a valuable tool in evaluation of dyspnea; it is rapid, generally reliable, and accurate. It is considerably more sensitive to hypoxia than the physician's clinical impression.26
Healthy individuals should have an oxygen saturation of at least 95% or greater. Many smokers, elderly
patients, and obese patients maintain oxygen saturations between 92% and 95%. Lower levels in a dyspneic patient require an explanation and often further diagnostic testing if the etiology of hypoxia remains in doubt. For select patients, an arterial blood gas (ABG) may provide additional information.
Emergency physicians can use pulse oximetry to measure oxygen saturation before and after
having a patient walk or exercise. A drop in oxegen saturation with exercise is characteristic of Pneumocystis carinii pneumonia.27
Pulse oximetry may also aid in treatment decisions. Patients with low levels require supplemental oxygen (although those with a significant shunt may not show improvement). A pulse oximetry reading of less than 90% suggests the need for admission in a patient with pneumonia, regardless of other factors.28
Limitations Of Pulse Oximetry. Despite the usefulness of pulse oximetry, the emergency physician must remain aware of its limitations. Pulse oximetry may be unobtainable in patients with shock, hypothermia, or severe vasoconstriction. It cannot detect abnormal hemoglobins that occur in patients with carbon monoxide toxicity or in those with methemoglobin. Pulse oximetry gives a false reading in cases of optical shunt. With sensor misplacement, the oximeter's light may not pass completely through the patient's finger, but may shine directly into the light receiver, creating an optical shunt. In this case, the monitor will not show a normal waveform.
Pulse oximetry measures oxygen saturation; it does not evaluate ventilation. Pulse oximetry cannot detect hypercarbia and impending respiratory failure, especially if the patient is given given supplemental oxygen. Do not exclude PE based on a normal pulse oximetry value. Oxygen saturation may be normal in a quarter of patients with PE.16
Chest radiography is a high-yield study in many patients with unexplained dyspnea. An anterior posterior (AP) or posterior anterior (PA) film plus a lateral projection provides a better view of chest structures than the portable AP study. In a prospective study of 221 ambulatory patients with cardiorespiratory complaints, chest x-ray demonstrated significant new abnormalities in more than one-third of patients.29 The most common abnormality was pulmonary infiltrate (18%).
Chest films are useful to determine the cause of unexplained dyspnea and the severity of suspected
etiologies. In pneumonia, they can detect high-risk findings such as pulmonary effusions, multi-lobar
disease, and cavitation. A normal film essentially rules out clinically significant pneumothorax. Chest radiography is invaluable in the diagnosis of congestive heart failure. Chest radiography combined with clinical assessment is 85% sensitive and 92% specific in detecting systolic dysfunction compared to echocardiography.30
Limitations Of Chest Radiography. Findings on chest films may be new or old, and without prior films,
this distinction may be impossible to make. The film may lag behind the clinical examination in many acute conditions, especially in adult respiratory distress syndrome (ARDS). While the chest x-ray provides important clues for PE, it may also obscure the diagnosis. The only time the chest film can exclude PE is when it demonstrates an incontrovertible alternative diagnosis (e.g., a pneumothorax). (Even then, it is possible for a truly unfortunate patient to have both diagnoses.) Significantly, it is impossible for a radiologist or emergency physician to distinguish PE from pneumonia on a chest film.18
A patient with a history of asthma or COPD does not routinely need a chest film. Chest x-rays may be necessary in patients who fail ED therapy and in those for whom a competing diagnosis is likely, such as concurrent pneumonia or CHF.31,32
Electrocardiography is particularly helpful in dyspneic patients with risk of cardiac disease. Myocardial ischemia is an important cause of painless dyspnea. Elderly patients and those with diabetes are likely to have atypical presentations of cardiac ischemia, especially shortness of breath.33 The electrocardiogram (ECG) may be positive in other causes of cardiac dyspnea, such as CHF, pericardial effusion, pulmonary hypertension, or rhythm disturbances.
Which patients with dyspnea need an ECG? Order an ECG for unexplained dyspnea in patients at risk for cardiac conditions. Although this population is not strictly defined, it may include men over age 35, postmenopausal women, and patients with ischemic risk factors such as hypertension, diabetes, family history of myocardial infarction, and especially those with prior cardiac disease. Dyspnea related to cardiac ischemia might be painless or can be accompanied by discomfort in the chest, jaw, neck, back, arms, or upper abdomen.
Evaluate the 12-lead ECG for evidence of myocardial ischemia, rate or rhythm disturbance, and evidence of hypertrophy. Atrial fibrillation can produce dyspnea by reducing cardiac output.
Left ventricular hypertrophy combined with elevations in the diastolic pressure suggests the possibility of left ventricular dysfunction. Electrocardiography improves the specificity of the physical exam in patients suspected of congestive heart failure. Clinical assessment alone is 41% sensitive for CHF, compared to 69% when ECG is incorporated. A normal ECG makes heart failure an unlikely diagnosis in the breathless patient, as a normal ECG has a 98% negative predictive value for left ventricular systolic dysfunction.18
Electrocardiography is rarely helpful in the diagnosis of PE. However, one study showed that symmetric Twave inversion in lead V1-4 was 85% sensitive and 81% specific for PE-but most of these patients had massive emboli.34 The famous S1 Q3 T3 pattern (often used to harass physicians in training) was only 54% sensitive for PE. In this study, no patients with submassive PE had sinus tachycardia.
Peak expiratory flow rates (PEFR) may be helpful in the emergency evaluation of the dyspneic patient. The following are several ccirumstances in which PEFRs are used in the ED:
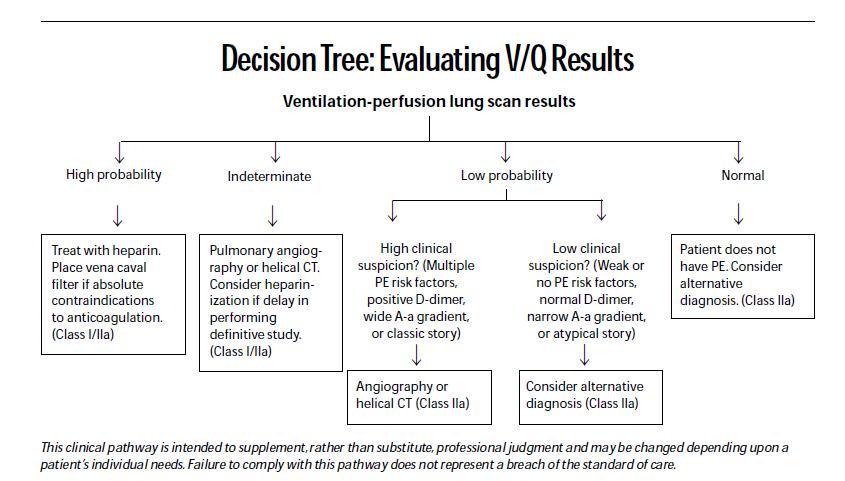
The ventilation perfusion (V/Q) lung scan is traditionally used to screen for PE.40 While a completely normal perfusion scan nearly eliminates this diagnosis, such a finding is rare. Most scans are indeterminate.
The V/Q scan has numerous limitations, and the terminology is misleading. A low-probability scan is a misnomer-angiography will demonstrate PE in as many as 12% of these patients.41 As many as 40% of patients with high pretest probablility and "low-probability scans" may have pulmonary emboli.42,43 When an emergency physician strongly suspects PE on clinical grounds, he or she should order additional tests for PE-despite a low-probability scan.
To effectively use the V/Q scan, the emergency physician must determine the clinical likelihood for PE before receiving the radiologist's reading. (See Table 4.) The pretest probability of PE remains a gestalt, and no validated scoring system yet exists.

If the clinical suspicion is discordant with the reading (low suspicion but high-probability scan, or high suspicion but low-probability scan), additional testing is needed. Any patient with a moderate probability or indeterminate scan requires additional testing.
Arterial blood gases (ABGs) are not routinely necessary for the dyspneic patient. In the COPD or asthmatic patient, a peak flow of 25% or greater than predicted may obviate the need for ABG. In many patients, pulse oximetry alone may be sufficient.
ABGs are useful in patients who have altered mental status and in those suspected of acidosis. Other indications include persistent hyperventilation, patients who are critically ill, and those with impending ventilatory failure.
In patients with unexplained dyspnea, the arterial alveolar gradient (A-a DO2 ) provides significant information. This number represents the gap between the partial pressure of oxygen in the alveolus and the partial pressure of oxygen in the blood. The wider the A-a DO2 gradient, the more significant the physiologic impairment. There is both a rigorous and a simple way to calculate the A-a DO2 gradient. (See Table 5 for the fancy way.) For quick determination of the A-a DO2 gradient at sea level, use the formula 150 minus 1.25 times PCO2 minus PO2 (A-a DO2=150 - 1.25 x PCO2 - PO2).

The A-a DO2 gradient normally increases with age. To adjust for age, use the following formula to give the expected age-appropriate gradient: patient age divided by four, plus four (adjusted normal for age=age/4 + 4).44 Thus, a 40-year-old smoker should have an A-a DO2 gradient of 14 mmHg.
The baseline A-a DO2 gradient increases in smokers and those with intrinsic lung disease such as COPD. It can only be determined accurately in a patient who is breathing room air, as the FIO2 on supplemental oxygen can only be estimated.
Determine the hemoglobin concentration in patients at risk for anemia. Such patients include those with melanotic stool, heavy vaginal bleeding, recent chemotherapy, history of AIDS, or recent trauma or surgery. Pale conjunctiva may suggest this diagnosis on physical examination. A fingerstick hemoglobin will suffice for most patients in whom anemia is a consideration.
Additional tests may provide important information in patients in whom standard studies are unrevealing. Most of these additional tests focus on the heart and lungs. Patients with persistent tachycardia and dyspnea may need evaluation for thyrotoxicosis.9
When the emergency physician continues to suspect cardiac disease due to a combination of risk factors or clinical exam, consider exercise testing or myocardial perfusion imaging.10,11
Echocardiography is becoming more accessible in emergency care. Transthoracic echo is very sensitive to pericardial effusion, even in the hands of a novice. Other findings such as valvular dysfunction and wall motion abnormalities require extensive training and sophisticated equipment.
Most patients with congestive failure can be diagnosed on clinical grounds coupled with chest radiography and ECG. Emergent echocardiography may help distinguish patients in whom the diagnosis of congestive failure vs. PE remains unclear.
Patients with congestive failure should have stigmata of left ventricular dysfunction, while those with significant PE may have right ventricular hypokinesis, dilatation of the right ventricle, or tricuspid regurgitation. Crawford and Hendry reported that clinical impression coupled with radiological findings was only 74% sensitive and 54% specific for systolic dysfunction in 61 patients with suspected heart failure.45 Echocardiography in these same patients led to important changes in management. They discovered three cases of cor pulmonale and 10 cases of valvular or pericardial disease.
Among patients with suspected PE, overall sensitivity for trans-thoracic echo in four prospective studies (n=317) was 80%, while specificity was 85%.46-49 In these studies, echocardiography assisted in the distinction between PE and congestive heart failure.
Pulmonologists may perform the methacholine challenge test in patients suspected of having atypical presentations of asthma. Other sophisticated pulmonary tests include the single-breath carbon monoxide diffusion test for interstitial lung disease.
Surely, no topic evokes such spirited debate as how to screen for PE. Every test seems to have as many drawbacks as advantages. Fortunately, diagnostic options available to the emergency physician are expanding.
The helical CT is able to image pulmonary vasculature as well as other thoracic structures. There are nine studies that use pulmonary angiography as a gold standard (n=371),50-58 and four that use other criteria to diagnose PE (n=611).59-63 The pooled sensitivity was 86% and the specificity was 93% for PE in these studies.
In the near future, refinements in helical CT may make computer tomography a test of choice for PE. However, at the current time, helical CT is most accurate for large central emboli and is insensitive for small peripheral clots.
The emergency physician should order helical CT for patients with suspected emboli who are likely to have non-diagnostic V/Q scans. This includes those with COPD, heavy cigarette use, sarcoidosis, pulmonary fibrosis, or those with an infiltrate on chest radiograph.64 Patients with an infiltrate on chest x-ray will have a non-diagnostic V/Q scan 82% of the time.64 A V/Q scan is likely to waste time and money in a pateint with focal consolidation.
D-dimer is a product of blood clot breakdown that rises in patients with thromboembolism. However, it is also elevated in patients with infection and those with inflammatory or neoplastic conditions. There are multiple commercial assays available for D-dimer, and four may be performed in less than one hour-some at the bedside.
The tests include:
Most of these assays are positive when the D-dimer concentration is more than 500 ng/mL.
The SimpliRED assay is the most extensively studied and probably most user-friendly test for ED evaluation.65 Five studies of the SimpliRED assay (n=1376) show a pooled average sensitivity of 90% and specificity of 60% for PE.65,67,69,102-104 The turbidimetric assays have also shown good test performance in three studies (n=684), with a sensitivity of 98% and a specificity of 43%.66-68
In one study, the combination of any two of the following-a normal SimpliRED D-dimer, a PO2 of 80 mmHg or more, or a respiratory rate less than 20-was unlikely to miss a pulmonary embolism.69 No patient with a normal SimpliRED test, a PO2 of 80 mmHg or greater, and a respiratory rate less than 20 had a PE in this trial.
The new-generation D-dimer assays are useful adjuncts to standard clinical criteria. They are probably best suited to the outpatient setting, where there may be fewer false-positives due to the lack of comorbid disease. In low-risk patients, a negative D-dimer assay can significantly lower the probability of PE. A negative D-dimer in conjunction with a low clinical probability provides a negative predictive value of 97%.65 Do not use the latex agglutination assays, as their sensitivity is poor (71%).67,70-72
Missed PE represents a dangerous event for both patients and physicians. Most cases of fatal PE go unrecognized before death.73 Contrary to the expectations of many practitioners, PE may present with isolated dyspnea.74-76
Isolated dyspnea is one of the most common symptoms in ambulatory patients with PE.40 In ED patients with PE, one-third report dyspnea without chest pain. This may be due to the fact that nearly half of ambulatory patients with PE have multiple emboli that do not result in lung infarction. Lung infarction is the primary cause of the pain associated with PE.77
In contrast, most hospitalized patients with PE (80- 90%) have painful dyspnea.18,78 This pulmonary infarction syndrome, characterized by painful dyspnea (and often hemoptysis), will usually demonstrate an infiltrate on chest x-ray.18
In a study of ambulatory patients, only two out of 26 of those with PE had symptoms and radiographic findings consistent with pulmonary infarction, compared to the 70-90% of hospitalized patients with PE.77,78
The diagnosis of PE is difficult for many reasons, not the least of which is its variable presentation. Some patients may have dramatic findings such as cyanosis and shock, while others may present with mild dyspnea. 79 Few bedside tests can eliminate the diagnosis of PE. Patients may have a normal PO2 by pulse oximetry or arterial blood gas.
Even a normal A-a DO2 gradient does not rule out PE; 15% of patients with angiographically proven pulmonary emboli will have a normal gradient.40,80-82 Young patients with emboli are especially likely to demonstrate normal oxygenation. In patients younger than 40 years of age, nearly 25% will have a normal A-a DO2 gradient.83 The A-a DO2 gradient is normal in more than half of pregnant patients with emboli.84 In older patients, the age-adjusted A-a DO2 gradient is 94% sensitive for PE but only 9% specific.83
A chest film is necessary in all patients with suspected PE. It helps the radiologist interpret other studies, such as the V/Q scan, and may provide an alternative diagnosis (pneumothorax). Nearly 80% of patients with PE have abnormal chest films.85 The most common findings include pleural effusion and infiltrate.
The V/Q scan is the most well-validated screening test for PE. A high-probability scan in conjunction with a high clinical probability is 97% specific for PE.41 If the perfusion portion of the scan is homogeneous (normal), regardless of the ventilation pattern, it excludes PE.41 Note the word "normal." Minor abnormalities or "nearnormal" scans do not have this sensitivity.
Acute bronchitis is defined as cough productive of sputum in a patient with no history of chronic lung disease and in whom the PEFR is near the predicted normal value. Acute bronchitis usually does not produce hypoxemia in an otherwise healthy person.
On occasion, purulent bronchitis can lead to mucus plugging and shunt, as demonstrated by a small series of patients studied with V/Q scanning.86 When mucus plugging is severe, treatment with a b2-agonist agent can transiently worsen oxygen saturation. This is because the b2-agonist produces pulmonary vasodilation in areas of non-ventilated lung, thus increasing shunt. However, patients may symptomatically feel better as the work of breathing is diminished.
Physicians have long recognized the syndrome of painless dyspnea due to myocardial ischemia. It has even been termed "blockpnea."87 Painless dyspnea often precedes angina in patients with significant coronary artery disease. In one study of British men with moderate-to-severe painless dyspnea, nearly 30% developed coronary artery disease within five years.88 The presumed mechanism for this ischemic dyspnea is impaired left ventricular contraction, diastolic dysfunction, and reduced lung compliance. These findings may underscore the importance of provocative cardiac testing in patients at risk for coronary artery disease who experience unexplained dyspnea.
Pregnancy certainly complicates the evaluation of dyspnea. Sixty to seventy percent of healthy women experience physiological dyspnea during pregnancy.89 However, pregnancy is a risk factor for two serious causes of dyspnea-eclampsia and PE. Pulmonary embolism is one of the leading causes of pregnancyrelated mortality and is responsible for 15% of all maternal deaths.83,90,91
Several mechanisms may cause physiologic dyspnea, including postural-dependent alterations in lung blood flow and increased sensitivity to CO2.89 However, dyspnea greater than 6 out of 10 on the Borg scale indicates a significant pathological process.15 The emergency physician must not overlook the diagnosis of PE in pregnancy. Fears of harm to the fetus from a ventilation-perfusion scan are misplaced. Dangers of untreated PE to both mother and fetus far outweigh the risks of radiation from either a V/Q scan or angiogram. 92,93 While consultation with an obstetrician is not inappropriate, emergency physicians must order the necessary tests if they suspect PE. The examining physician has a far better understanding of the need for such tests than a consultant called at home.
Fetal exposures can be reduced by placing a lead apron over the uterus during the chest x-ray and performing a half-dose perfusion scan without the ventilation component.94,95 A normal perfusion scan will rule out the diagnosis of PE.
The emergency physician can usually determine the presence of heart failure based upon the clinical examination and a few simple tests. Physician judgment is quite accurate in excluding the diagnosis. If the emergency physician does not believe the patient clinically has congestive heart failure, and the chest radiograph and ECG are both normal, then the dyspnea is not due to CHF.30
A history of congestive heart failure does not mean the current episode of dyspnea is due to an exacerbation of failure. PE is a significant cause of mortality in patients with CHF. One multi-center study shows that a history of congestive heart failure doubled the death rate from PE.96 Pulmonary embolism in patients with a history of congestive heart failure may be indistinguishable from an exacerbation of CHF.18,75
Historical factors may help distinguish the two conditions; patients who stop taking their cardiac medications and those who complain of progressive orthopnea and weight gain are more likely to have failure. The patient with acute dyspnea remains at risk of embolism.
Unfortunately, no specific bedside tests can reliably distinguish a patient with acute PE and prior CHF from a patient with a simple exacerbation of congestive heart failure. The chest radiograph is helpful, as radiographic evidence of lung edema is 95% sensitive for failure.30 Isolated PE is unlikely to produce such a finding.74,83 Liberal use of V/Q scans, echocardiography, or helical CT may be necessary in dyspneic patients with a history of CHF and relatively normal chest films.97
Transthoracic echocardiography may distinguish congestive heart failure from PE. Finally, the PEFR can help differentiate CHF from obstructive airway disease as a cause of dyspnea.35
Psychogenic dyspnea is synonymous with psychogenic hyperventilation. It is seen in young people with no identifiable organic cause. The etiology is multifactorial and may overlap with panic disorder. Both disorders may be related to heightened sensitivity to arterial PCO2.98
Panic attacks usually come without warning and are not necessarily precipitated by a stressful situation. Patients experiencing a panic attack may complain of a lump in their throat (globus hystericus) or that their clothes or undergarments are too tight. There are several characteristic types of panic attacks. The unexpected panic attack occurs spontaneously, without a situational trigger. The situational-bound panic attack occurs upon exposure to a frightening stimulus (seeing a snake, dog, or other frightening trigger).99
The diagnosis of psychogenic dyspnea in the ED should be a diagnosis of exclusion. It is best reserved for young, healthy patients with a history of previous attacks. The diagnosis of a new-onset panic attack or hyperventilation syndrome in an older adult invites tragedy and litigation. (See also the "Ten Excuses That Don't Work In Court".)
When discharging the patient with presumed psychogenic dyspnea, avoid premature closure in diagnosis. The ED diagnosis may reflect "dyspnea, etiology unknown," and the differential diagnosis may include psychogenic dyspnea. Patients with psychogenic dyspnea may respond to anxiolytics.100
The deconditioning syndrome occurs in patients with exertional dyspnea without organic etiology. patients are usually greater than 30% over the ideal body weight for height and have a sedentary lifestyle. Psychogenic dyspnea may account for 32% of unexplained shortness of breath, while deconditioning is responsible for another 28%.10 Among young ambulatory patients with a normal evaluation, as many as half of the subjects may have psychogenic dyspnea or deconditioning syndrome.10-12,100 Such patients are not expected to have a low pulse oximetry, abnormal chest x-ray, or abnormal vital signs. Deconditioning may improve after exercise and weight loss protocol (an endpoint difficult to achieve during an ED visit).
The treatment and disposition of patients with the myriad causes of dyspnea is beyond the scope of this article. However, a few points are in order.
Patients with respiratory distress need a rapid evaluation of their airway. Patients with altered mental status, inability to speak, or inadequate ventilations may require airway management. While intubation remains the most definitive airway, some dyspneic patients not in extremis may benefit from noninvasive positive pressure ventilation (BiPAP or CPAP). Research continues on the use of alternative gases such as heliox for patients with upper airway obstruction or asthma.
Pulse oximetry is a helpful, early intervention. It is sensitive to hypoxia and should trigger the administration of supplemental oxygen if the O2 saturation is less than normal.
Oxygen is good—even for patients with COPD who depend upon the hypoxic drive for ventilation. (See also the "Ten Excuses That Don't Work In Court" ) The only absolute contraindication to oxygen is acute paraquat toxicity.101 (I'll bet you didn't know that one!)
Sit the patient upright. The bolt-upright position maximizes accessory muscle use and may decrease pulmonary congestion in those with heart failure. Patients who are unable to sit upright because of shock or altered mental status may be placed in the supine position and intubated.
Do not discharge patients without attempting to explain the cause of the dyspnea. The evaluation may be as simple as a history and physical examination, or it could be complex and expensive.
Patients with dyspnea may have causes that range from the benign to catastrophic. In most cases of dyspnea, the history and physical examination, as well as a few bedside tests such as chest x-ray and pulse oximetry, will drive the scope of this evaluation. A dangerous pitfall is the failure to consider pulmonary embolism. Fortunately, several easily available tests can obviate the need for a lung scan, such as the new-generation D-dimer test in combination with the respiratory rate and/or the A-a gradient.
2. "But the pulse ox was normal!"
3. "But he had CHF the last time he came to the ED."
4. "Here it is right in the chart……No chest pain'!"
5. "I knew he was pulled out of a burning building…that's why I got the pulse ox."
6. "Even the radiologist said the chest film showed pneumonia."
7. "The radiologist said the chest x-ray was normal."
8. "After I gave him the high-flow oxygen, he calmed down a lot…he even went to sleep. So I turned out the lights and let him rest."
9. "I didn't get the V/Q scan because her obstetrician said she didn't need it."
10. "I should have ordered the chest x-ray and a pulse ox."
1. Limit ABGs.
ABGs are usually unnecessary in patients with asthma or COPD, especially if the PEFR is greater than 25% of the predicted value. If a patient has a normal pulse oximetry on room air, an arterial blood gas is not necessary to rule out hypoxemia.
2. Limit V/Q scans to patients likely to have PE.
A V/Q lung scan is usually unnecessary in a patient with a low clinical risk for PE and a normal new-generation D-dimer assay ( < 500 ng/mL).
3. Limit chest x-rays in asthma and COPD.
Patients with a prior history of asthma or COPD do not need a chest film for every ED visit. Limit radiography to patients who fail to improve despite adequate ED herapy or those with a likely comorbid condition such as pneumonia or pneumothorax.
4. Limit portable chest films to unstable patients.
Order PA and lateral chest x-rays in all but unstable patients. Portable AP films are more expensive and less accurate for pathology.
5. More metered-dose inhalers-fewer nebulizers.
Metered-dose inhalers with spacer chambers are at least as effective as hand-held nebulizers in the treatment of asthma and COPD-and are significantly less expensive.
6. Consider the helical CT.
Patients suspected of PE who have an infiltrate on chest x-ray are very likely to have a non-diagnostic V/Q scan. Consider a contrast-enhanced helical CT in such patients.





Evidence-based medicine requires a critical appraisal of the literature based upon study methodology and number of subjects. Not all references are equally robust. The findings of a large, prospective, randomized, and blinded trial should carry more weight than a case report.
To help the reader judge the strength of each reference, each reference will note (in bold type following the reference) pertinent information about the study, such as the type of study and the number of patients in the study. In addition, the most informative references cited in the paper, as determined by the author, will be noted by an asterisk (*) next to the number of the reference.
Jeffrey A. Kline
August 1, 1999
Accredited By





Our Partners


 678-366-7933
678-366-7933