|
|
Given the rising prevalence of obesity and the expanding use of weight-loss treatments, urgent care clinicians must be prepared to recognize and manage potential adverse effects. The most common complaints include nausea, vomiting, diarrhea, and abdominal discomfort, though each medication class carries specific risks and complications. Management strategies vary depending on the medication used and the severity of symptoms. In some cases, discontinuation or dose adjustment may be necessary, while severe complications such as dehydration or pancreatitis may require emergency evaluation. This review provides an overview of the most prescribed weight-loss medications, highlights their potential side effects and complications, and offers evidence-based recommendations for patient management and disposition.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
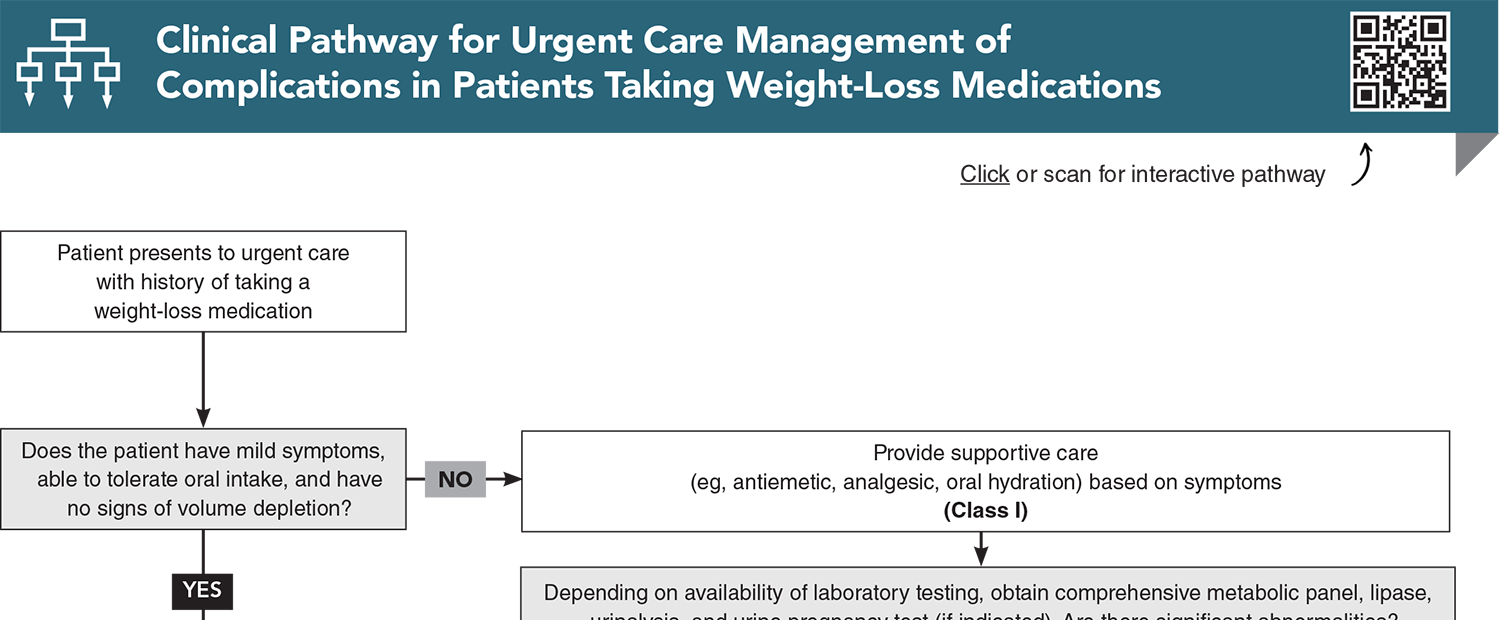
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
2. * Yanovski SZ, Yanovski JA. Approach to obesity treatment in primary care: a review. JAMA Intern Med. 2024;184(7):818-829. (Clinical review) DOI: 10.1001/jamainternmed.2023.8526
3. * DeCleene NK, Kahn E, Yuan CW, et al. US state-level prevalence of adult obesity by race and ethnicity from 1990 to 2022 and forecasted to 2035. JAMA. 2026: e2526817. (Survey data) DOI: 10.1001/jama.2025.26817
4. * Hampl SE, Hassink SG, Skinner AC, et al. Clinical practice guideline for the evaluation and treatment of children and adolescents with obesity. Pediatrics. 2023;151(2):e2022060640. (Practice guideline) DOI: 10.1542/peds.2022-060640 Pharmacotherapy for obesity-trends using a population level national database. Obes Surg. 2021;31(3):1105-1112. (Prospective database study)
6. * Yanovski SZ, Yanovski JA. Long-term drug treatment for obesity: a systematic and clinical review. JAMA. 2014;311(1):74-86. (Clinical review) DOI: 10.1001/jama.2013.281361
7. * Weghuber D, Barrett T, Barrientos-Perez M, et al. Once-weekly semaglutide in adolescents with obesity. N Engl J Med. 2022;387(24):2245-2257. (Randomized controlled trial; 180 participants) DOI: 10.1056/NEJMoa2208601
Subscribe to get the full list of 33 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: weight-loss medications, glucagon-like peptide-1 (GLP-1) receptor agonist, dual GLP-1/glucose-dependent insulinotropic polypeptide (GIP) receptor agonist, sympathomimetic amine, lipase inhibitor, obesity, drug reactions, semaglutide, liraglutide, tirzepatide, phentermine, phentermine-topiramate, orlistat, naltrexone-bupropion, Xenical®, Qysmia®, Contrave®, Saxenda®, Wegovy®, Zepbound®, gastrointestinal side effects, injection site reactions, constipation, pancreatitis, vomiting, nausea, diarrhea, hyperkalemia, dehydration, renal dysfunction, hypertension, tachycardia, antiobesity medications, oral hydration, antiemetic, analgesia
Hannah Caplan, DO, MSc; Tyler Johnson, MD; Hope Ring, MD, FACEP; Michelle Wilson, MD
Erin Loo, PA-C, MHA, FCUCM; Ajsa Nikolic, MD, MHA
April 1, 2026
Evidence-Based Urgent Care • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Evidence-Based Urgent Care issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933