

|
|
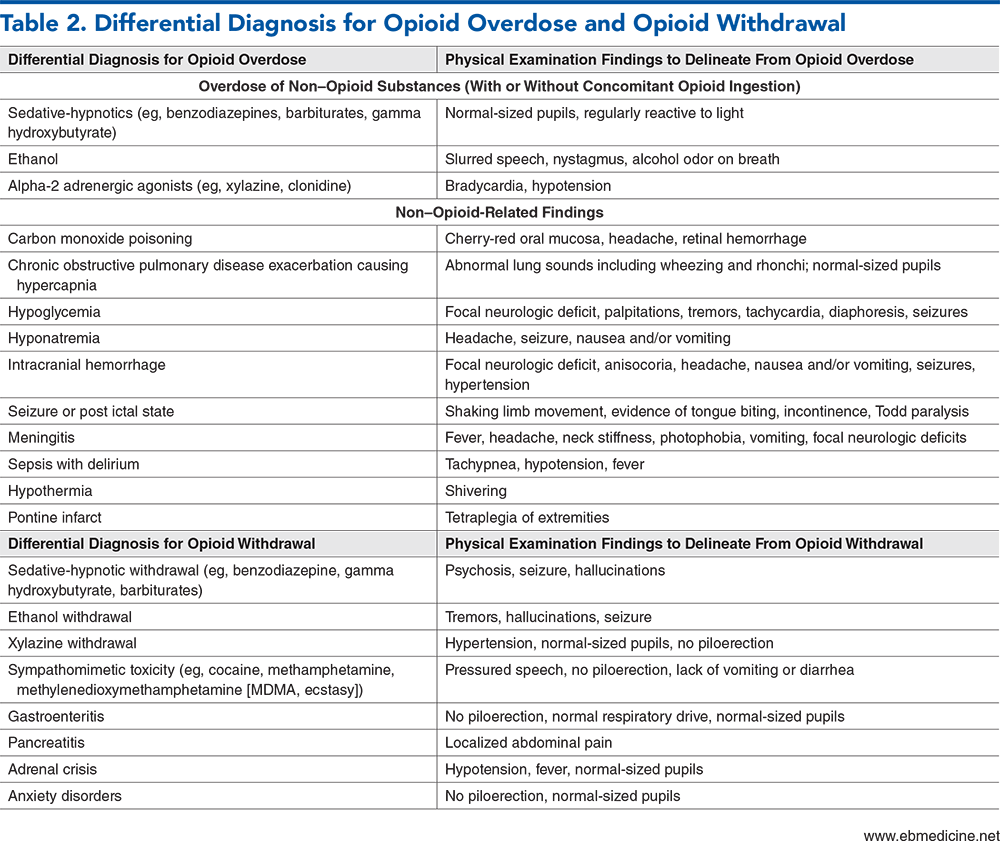
As the United States continues to grapple with the opioid crisis, emergency clinicians are on the front lines of managing patients with opioid use disorder. This issue reviews tools and best practices in emergency department management of patients with opioid overdose and opioid withdrawal, and how substance use history will inform treatment planning and disposition. As growing evidence shows that medications for opioid use disorder (MOUD)—buprenorphine, methadone, and naltrexone—can have lasting impacts on patients’ addiction recovery, strategies for assessing patient readiness for MOUD and overcoming barriers to emergency department initiation of these medications are reviewed. Newer approaches to buprenorphine dosing (high-dose, low-dose, home induction, and long-acting injectable dosing) are also reviewed.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
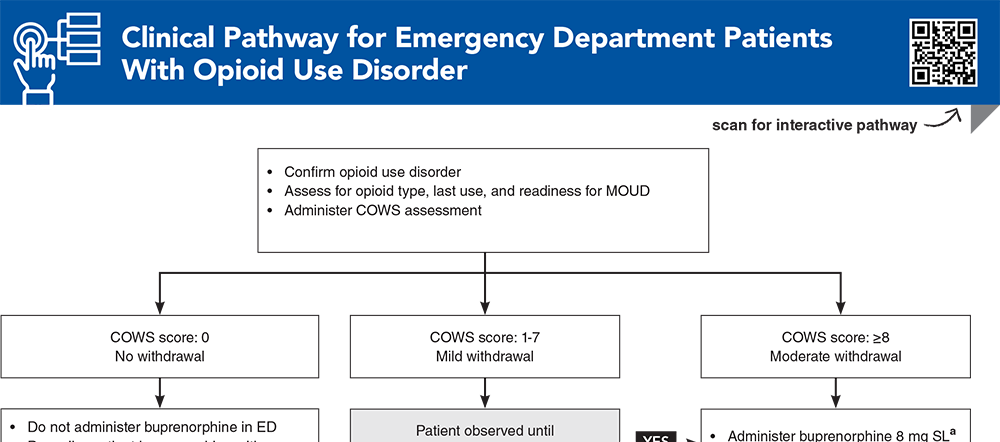
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Subscribe for full access to Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
10. * D’Onofrio G, O’Connor PG, Pantalon MV, et al. Emergency department-initiated buprenorphine/naloxone treatment for opioid dependence: a randomized clinical trial. JAMA. 2015;313(16):1636-1644. (Randomized control trial; 329 patients) DOI: 10.1001/jama.2015.3474
11. Moe J, Badke K, Pratt M, et al. Microdosing and standard-dosing take-home buprenorphine from the emergency department: a feasibility study. J Am Coll Emerg Physicians Open. 2020;1(6):1712-1722. (Randomized feasibility trial; 54 patients) DOI: 10.1002/emp2.12289
23. * Greenwald MK, Herring AA, Perrone J, et al. A neuropharmacological model to explain buprenorphine induction challenges. Ann Emerg Med. 2022;80(6):509-524. (Review article) DOI: 10.1016/j.annemergmed.2022.05.032
60. * Childers R, Castillo EM, Cronin AO, et al. Emergency department-initiated buprenorphine treatment in a population with a high rate of homelessness: an observational study. J Emerg Med. 2023;64(2):129-135. (Descriptive analysis; 210 patients) DOI: 10.1016/j.jemermed.2022.12.004
73. * Whiteside LK, D’Onofrio G, Fiellin DA, et al. Models for implementing emergency department-initiated buprenorphine with referral for ongoing medication treatment at emergency department discharge in diverse academic centers. Ann Emerg Med. 2022;80(5):410-419. (Project proposal and description) DOI: 10.1016/j.annemergmed.2022.05.010
87. * Snyder H, Chau B, Kalmin MM, et al. High-dose buprenorphine initiation in the emergency department among patients using fentanyl and other opioids. JAMA Netw Open. 2023;6(3):e231572. (Retrospective cohort study; 439 patients) DOI: 10.1001/jamanetworkopen.2023.1572
Subscribe to get the full list of 98 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: opioid, disorder, MOUD, withdrawal, overdose, methadone, buprenorphine, naloxone, naltrexone, fentanyl, xylazine, COWS
Corey S. Hazekamp, MD, MS; Dana Sacco, MD, MSc
Patrick Maher, MD, MS; Brian G. Wiener, MD
June 1, 2024
June 1, 2027 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits. Specialty CME Credits:Included as part of the 4 credits, this CME activity is eligible for 4 Substance Use Disorders CME credits, subject to your state and institutional approval. This CME activity is eligible for 4 credits toward the United States Department Justice Drug Enforcement Administration Medication Access and Training Expansion (MATE) requirements.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933
