|
|
Distinguishing viral from bacterial causes of pneumonia in the urgent care setting is paramount to providing effective treatment but remains a significant challenge. For pediatric patients who can be managed with outpatient treatment, the utility of laboratory tests and radiographic studies, as well as the need for empiric antibiotics, remains questionable. This issue reviews viral and bacterial etiologies of community-acquired pneumonia in pediatric patients, offers guidance for obtaining historical information and interpreting physical examination findings, discusses the utility of various diagnostic techniques, and provides recommendations for the treatment of previously healthy and medically fragile children.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
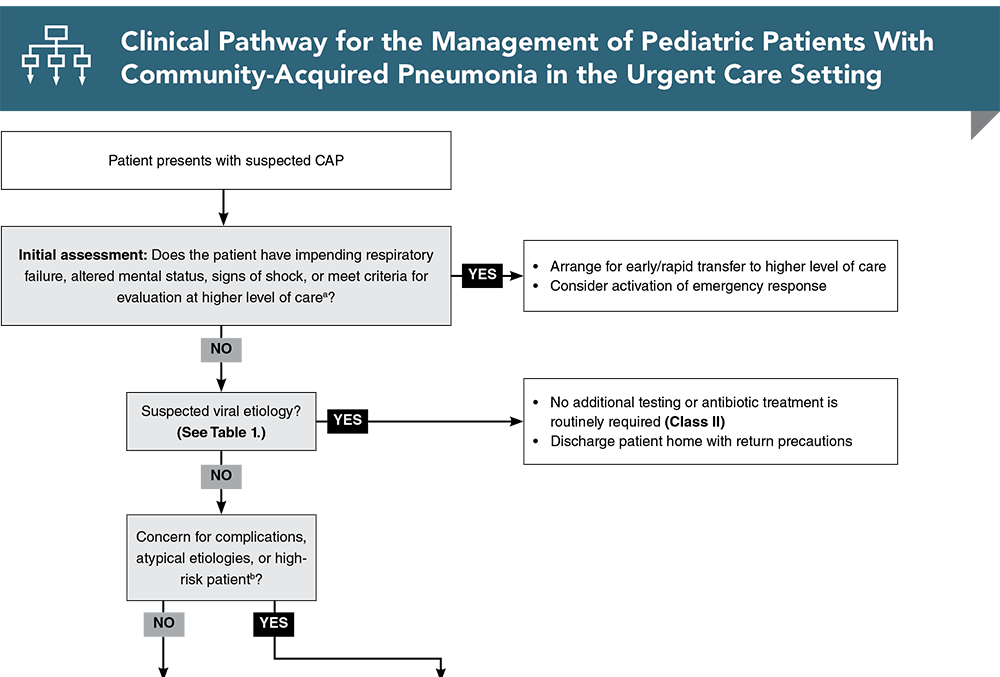
Subscribe to access the complete flowchart to guide your clinical decision making.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
1. * Kronman MP, Hersh AL, Feng R, et al. Ambulatory visit rates and antibiotic prescribing for children with pneumonia, 1994-2007. Pediatrics. 2011;127(3):411-418. (Population-based surveillance) DOI: 10.1542/peds.2010-2008
5. * Jain S, Williams DJ, Arnold SR, et al. Community-acquired pneumonia requiring hospitalization among U.S. children. N Engl J Med. 2015;372(9):835-845. (Prospective study; 2358 patients) DOI: 10.1056/NEJMoa1405870
10. * Korppi M, Don M, Valent F, et al. The value of clinical features in differentiating between viral, pneumococcal and atypical bacterial pneumonia in children. Acta Paediatr. 2008;97(7):943-947. (Case-control study; 101 patients) DOI: 10.1111/j.1651-2227.2008.00789.x
23. * Li ST, Tancredi DJ. Empyema hospitalizations increased in US children despite pneumococcal conjugate vaccine. Pediatrics. 2010;125(1):26-33. (Retrospective study; 2898 patients) DOI: 10.1542/peds.2009-0184
44. National Asthma Education and Prevention Program, Third Expert Panel on the Diagnosis and Management of Asthma. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. National Heart, Lung, and Blood Institute (US); 2007. Accessed December 10, 2023. (Guidelines)
49. * Shah SN, Bachur RG, Simel DL, et al. Does this child have pneumonia?: The rational clinical examination systematic review. JAMA. 2017;318(5):462-471. (Systematic review; 23 prospective cohort studies, 13,833 children) DOI: 10.1001/jama.2017.9039
54. * Bachur R, Perry H, Harper MB. Occult pneumonias: empiric chest radiographs in febrile children with leukocytosis. Ann Emerg Med. 1999;33(2):166-173. (Prospective cohort study; 278 patients) DOI: 10.1016/s0196-0644(99)70390-2
55. * Mathews B, Shah S, Cleveland RH, et al. Clinical predictors of pneumonia among children with wheezing. Pediatrics. 2009;124(1):e29-e36. (Prospective cohort study; 526 subjects) DOI: 10.1542/peds.2008-2062
73. * St Peter SD, Tsao K, Spilde TL, et al. Thoracoscopic decortication vs tube thoracostomy with fibrinolysis for empyema in children: a prospective, randomized trial. J Pediatr Surg. 2009;44(1):106-111. (Randomized controlled trial; 36 patients) DOI: 10.1016/j.jpedsurg.2008.10.018
123. *Bielicki JA, Stohr W, Barratt S, et al. Effect of amoxicillin dose and treatment duration on the need for antibiotic re-treatment in children with community-acquired pneumonia: the CAP-IT randomized clinical trial. JAMA. 2021;326(17):1713-1724. (Multicenter, randomized controlled trial; 824 patients) DOI: 10.1001/jama.2021.17843
Portions of this content were adapted from: Cooper-Sood J, Wallihan R, Naprawa J. Pediatric community-acquired pneumonia: diagnosis and management in the emergency department. Pediatr Emerg Med Pract. 2019;16(4):1-28 Used with permission of EB Medicine.
Subscribe to get the full list of 139 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: pediatric pneumonia, community-acquired pneumonia, CAP, pediatric CAP, viral pneumonia, bacterial pneumonia, mycoplasma pneumoniae, CXR, asthma, antibiotic, COVID, influenza, pleural effusion
Amanda Nedved, MD, FAAP
Jo Ann Beltre, MD, FAAP; Joseph D. Lynch, MD, FAAP, CHSE
January 1, 2024
January 1, 2027 CME Information
4 AMA PRA Category 1 Credits™. 4 AOA Category 2-B Credits. 4 AAFP Prescribed Credits Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 4 Infectious Disease and 1 Pharmacology CME credits.
Evidence-Based Urgent Care • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Evidence-Based Urgent Care issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933