|
|
Public health programs have helped decrease the prevalence and sequelae of measles, mumps, rubella, and varicella; however, misinformation regarding vaccinations and recent disruptions to vaccination programs have caused outbreaks to occur. Emergency clinicians must be able to readily identify the characteristic presentations of measles, mumps, rubella, and varicella, with the goals of optimizing supportive care, limiting the spread of disease, and giving appropriate precautionary advice for complications to patients and their families. This issue provides a review of the clinical features, differential diagnoses, potential complications, and treatment options for measles, mumps, rubella, and varicella.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
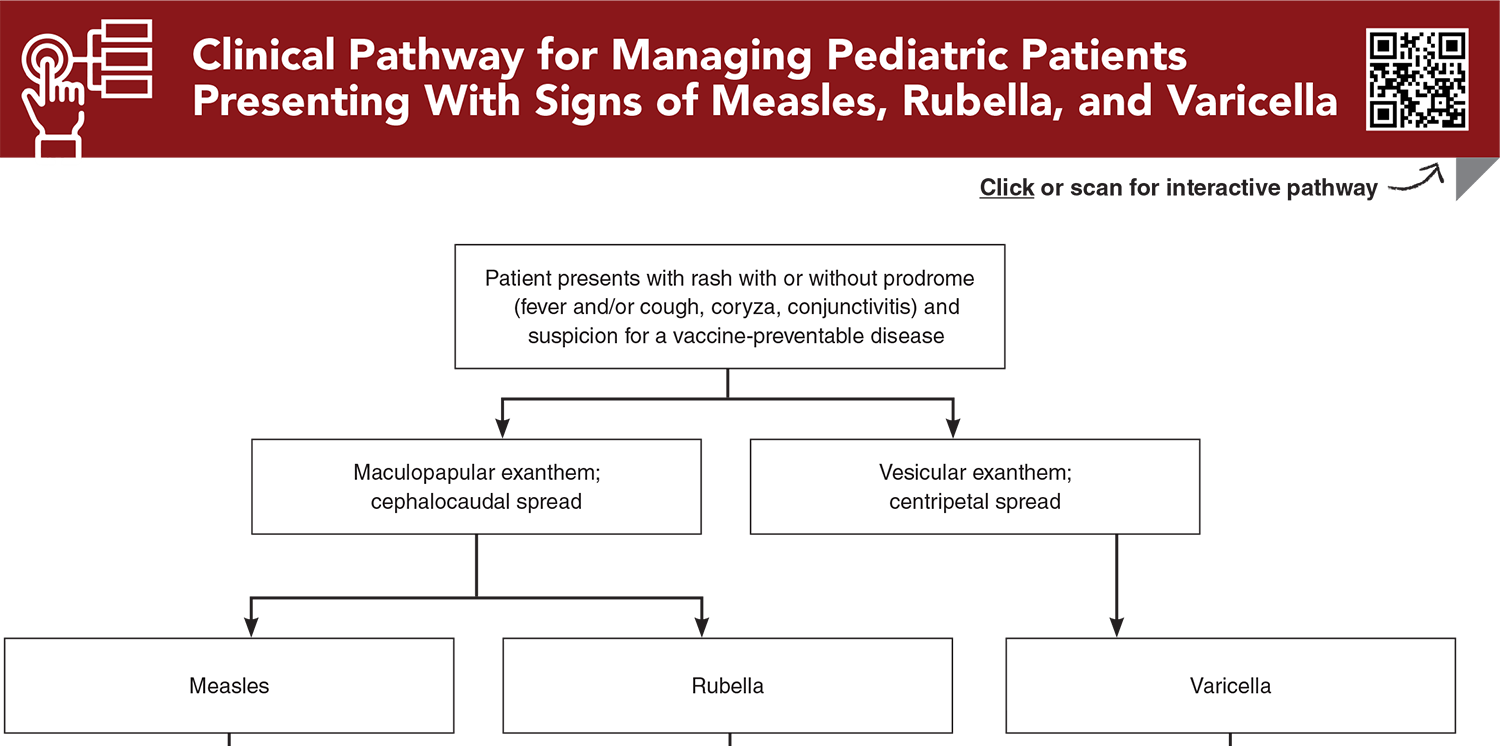
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
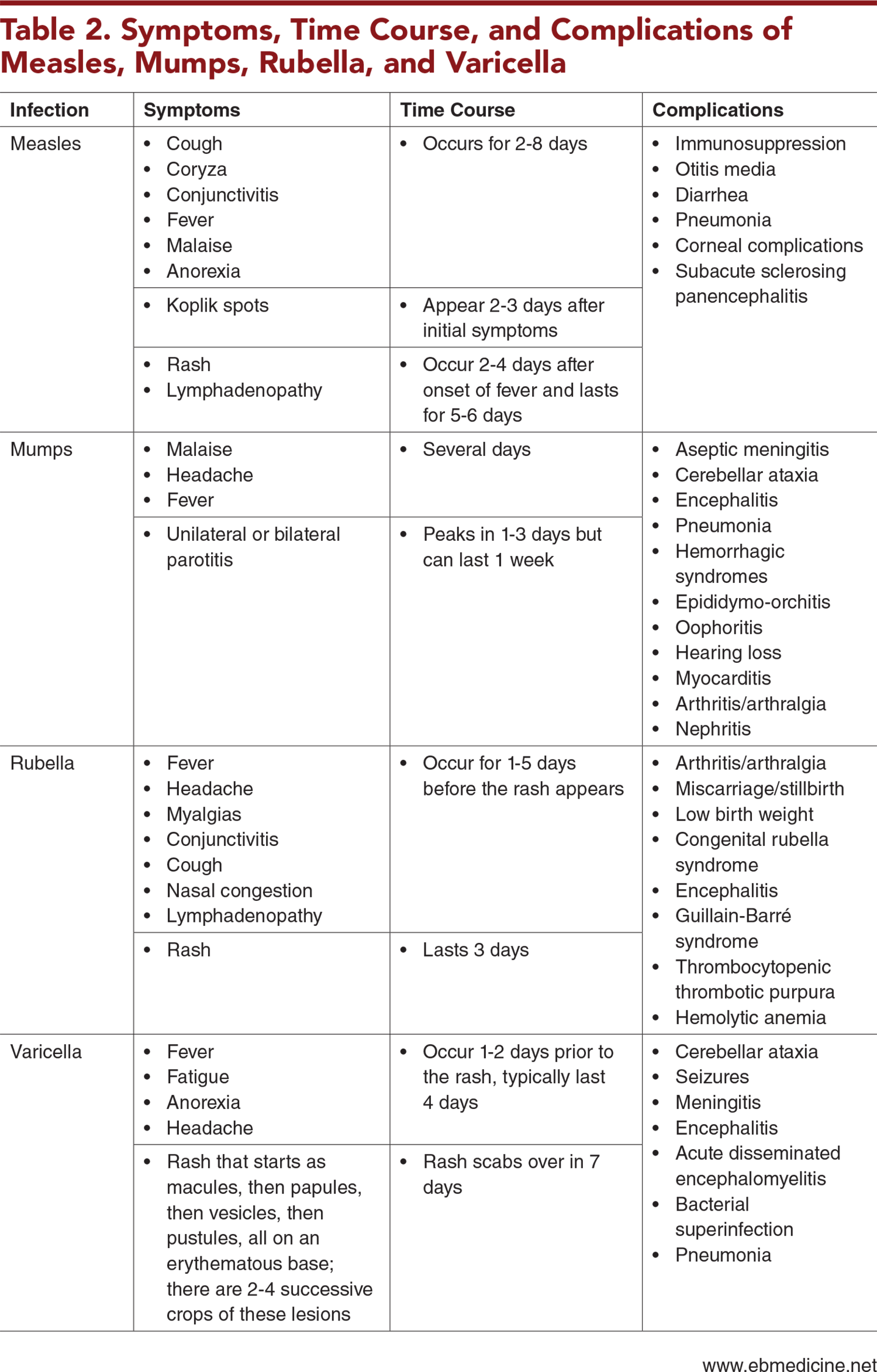
Subscribe for full access to all Tables, Figures, and Appendix.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
1. * Anderer S. Global measles cases rose 20% in 1 year as vaccine coverage fell short. JAMA. 2025;333(4):279. (Review) DOI: 10.1001/jama.2024.25514
11. * United States Centers for Disease Control and Prevention. Chickenpox (varicella). Chickenpox vaccination. 2025. Accessed October 1, 2025. (National recommendation)
14. * United States Centers for Disease Control and Prevention. Measles cases and outbreaks. 2025. Accessed October 1, 2025. (National recommendations)
17. * United States Centers for Disease Control and Prevention. Rubella (German measles, three-day measles): impact of U.S. MMR Vaccination Program. 2025. Accessed October 1, 2025. (National recommendations)
18. * Papania MJ, Wallace GS, Rota PA, et al. Elimination of endemic measles, rubella, and congenital rubella syndrome from the Western hemisphere: the US experience. JAMA Pediatr. 2014;168(2):148-155. (Expert review) DOI: 10.1001/jamapediatrics.2013.4342
19. * Marin M, Meissner HC, Seward JF. Varicella prevention in the United States: a review of successes and challenges. Pediatrics. 2008;122(3):e744-e751. (Review) DOI: 10.1542/peds.2008-0567
32. * Ziebold C, von Kries Rd, Lang R, et al. Severe complications of varicella in previously healthy children in Germany: a 1-year survey. Pediatrics. 2001;108(5):e79. (Surveillance study; 119 children) DOI: 10.1542/peds.108.5.e79
39. * American Academy of Pediatrics. Measles. In: Kimberlin D, Banerjee R, Barnett E, et al, eds. Red Book: 2024–2027 Report of the Committee on Infectious Diseases. 33rd ed. 2024:570-585. (Expert recommendations) DOI: 10.1542/9781610027373-S3_012_002
43. * American Academy of Pediatrics. Mumps. In: Committee on Infectious Diseases, Kimberlin D, Banerjee R, et al, eds. Red Book: 2024–2027 Report of the Committee on Infectious Diseases. 33rd ed. 2024:611-616. (Expert recommendation) DOI: 10.1542/9781610027373-S3_012_009
44. * American Academy of Pediatrics. Rubella. In: Committee on Infectious Diseases, Kimberlin D, Banerjee R, et al, eds. Red Book: 2024–2027 Report of the Committee on Infectious Diseases. 33rd ed.2024:735-741. (Expert recommendations) DOI: 10.1542/9781610027373-S3_017_009
46. * American Academy of Pediatrics. Varicella-zoster virus infections. In: Kimberlin D, Banerjee R, Barnett E, et al, eds. Red Book: 2024–2027 Report of the Committee on Infectious Diseases. 33rd ed.2024:938-951. (Expert recommendations) DOI: 10.1542/9781610027373-S3_021_001
53. * Black S, Shinefield H, Ray P, et al. Postmarketing evaluation of the safety and effectiveness of varicella vaccine. Pediatr Infect Dis J. 1999;18(12):1041-1046. (Retrospective case control; 89,753 patients) DOI: 10.1097/00006454-199912000-00003
64. * Demicheli V, Rivetti A, Debalini MG, et al. Vaccines for measles, mumps and rubella in children. Cochrane Database Syst Rev. 2012;2012(2):CD004407. (Systematic review; 58 studies, 14,700,00 patients)
Subscribe to get the full list of 66 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: measles, mumps, rubella, varicella, vaccine-preventable disease, vaccine-preventable illness, disease outbreak, rubeola, 3-day measles, German measles, congenital rubella syndrome, varicella-zoster, herpes zoster, shingles, viral disease, pediatric infections, vaccine, vaccination, vaccine hesitancy, vaccine refusal, MMR vaccine, MMRV vaccine, reporting, isolation precautions, postexposure prophylaxis, antiviral therapy, vaccine adverse events, vaccination schedule, contact exposure
Sarah C. Cavallaro, MD
Sylvia Owusu-Ansah, MD, MPH, FAAP; Lara Zibners, MD, MMEd, MBA
November 1, 2025
November 1, 2028 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAP Prescribed Credits, 4 AOA Category 2-B Credits. Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 4 Infectious Disease CME credits and 1 Pharmacology CME credit, subject to your state and institutional approval.
Pediatric Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Pediatric Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933