
|
|
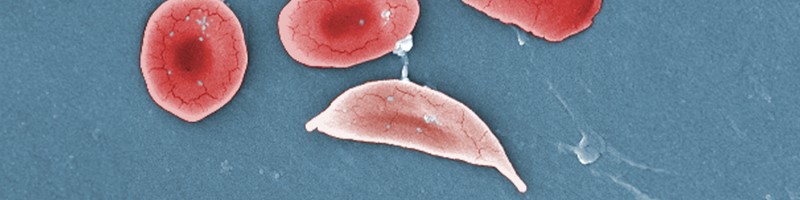
Sickle cell disease is a chronic hematologic disease that affects over 100,000 people in the United States. Many of these patients will present to the emergency department seeking treatment for an acute complication. Vaso-occlusive crisis, the most common recurring complication, can be difficult to manage because of the stigma patients face surrounding management of their pain. Patients with sickle cell disease presenting with conditions such as pain, infection, respiratory distress, stroke, or priapism must be given special consideration, as management can differ from that of the general population. This review evaluates the current guidelines and literature on acute complications related to sickle cell disease to dispel misconceptions about seemingly harmless interventions and provide clarification on those that are more controversial. Novel treatments that may have future impact on the management of patients with sickle cell disease are also reviewed.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.

Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
3. * Brandow AM, Carroll CP, Creary S, et al. American Society of Hematology 2020 guidelines for sickle cell disease: management of acute and chronic pain. Blood Adv. 2020;4(12):2656-2701. (ASH guidelines) DOI: 10.1182/bloodadvances.2020001851
4. * National Heart, Lung, and Blood Institute, Buchanan GR, Yaw BP, co-chairs. Evidence-based management of sickle cell disease: expert panel report, 2014. Accessed July 11, 2024. (NHLBI Expert Panel report)
5. * Freiermuth C, Kavanagh P, Bailey L, et al. Sickle cell. 2023. Accessed July 11, 2024. Available at: https://poctools.acep.org/POCTool/SickleCell/df0c5789-695b-4ceb-8fde-9f3db269a26d/ (Online point-of-care tool)
23. * Walter O, Cougoul P, Maquet J, et al. Risk of vaso-occlusive episode after exposure to corticosteroids in patients with sickle cell disease. Blood. 2022;139(26):3771-3777. (Case-control; 5151 patients) DOI: 10.1182/blood.2021014473
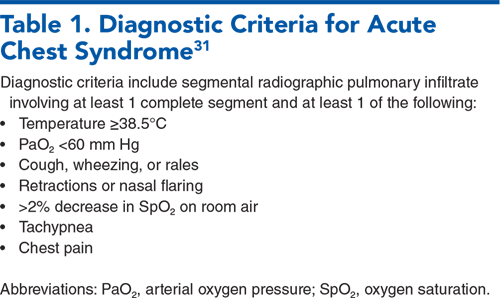
33. * Vichinsky EP, Neumayr LD, Earles AN, et al. Causes and outcomes of the acute chest syndrome in sickle cell disease. National Acute Chest Syndrome Study Group. N Engl J Med. 2000;342(25):1855-1865. (Retrospective; 671 episodes of ACS) DOI: 10.1056/NEJM200006223422502
42. * Ohene-Frempong K, Weiner SJ, Sleeper LA, et al. Cerebrovascular accidents in sickle cell disease: rates and risk factors. Blood. 1998;91(1):288-294. (Prospective; 4082 patients) DOI: 10.1182/blood.V91.1.288
56. * Rineer S, Walsh PS, Smart LR, et al. Risk of bacteremia in febrile children and young adults with sickle cell disease in a multicenter emergency department cohort. JAMA Netw Open. 2023;6(6):e2318904. (Retrospective; 1118 patients) DOI: 10.1001/jamanetworkopen.2023.18904
68. * Zempsky WT. Treatment of sickle cell pain: fostering trust and justice. JAMA. 2009;302(22):2479-2480. (Commentary) DOI: 10.1001/jama.2009.1811
73. * Elmariah H, Garrett ME, De Castro LM, et al. Factors associated with survival in a contemporary adult sickle cell disease cohort. Am J Hematol. 2014;89(5):530-535. (Prospective; 542 patients) DOI: 10.1002/ajh.23683
85. * Bellet PS, Kalinyak KA, Shukla R, et al. Incentive spirometry to prevent acute pulmonary complications in sickle cell diseases. N Engl J Med. 1995;333(11):699-703. (Randomized controlled trial; 29 patients) DOI: 10.1056/NEJM199509143331104
106. *Morris CR, Kuypers FA, Lavrisha L, et al. A randomized, placebo-controlled trial of arginine therapy for the treatment of children with sickle cell disease hospitalized with vaso-occlusive pain episodes. Haematologica. 2013;98(9):1375-1382. (Randomized controlled trial; 38 patients) DOI: 10.3324/haematol.2013.086637
Subscribe to get the full list of 110 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: sickle cell, vaso-occlusion, VOC, acute chest, priapism, splenic, transfusion, sepsis, opioid
Babette Newman, DO; R. Gentry Wilkerson, MD
Caroline Freiermuth, MD, MHS, FACEP; Angela Hua, MD, FACEP
August 1, 2024
August 1, 2027 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933