|
|
Pelvic inflammatory disease is associated with complications that include infertility, chronic pelvic pain, ruptured tubo-ovarian abscess, and ectopic pregnancy. When only nonspecific signs and symptoms are present at clinical evaluation, the diagnosis may be delayed. Even when properly diagnosed, pelvic inflammatory disease is often treated in a suboptimal manner. This review provides evidence-based recommendations for the diagnosis, treatment, disposition, and follow-up of patients with pelvic inflammatory disease. Emerging issues, including new pathogens and evolving resistance patterns among long-established pathogens, are also reviewed.
A 30-year-old woman presents with lower abdominal pain...
A 22-year-old woman returns for re-evaluation 1 week after starting treatment for pelvic inflammatory disease...
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
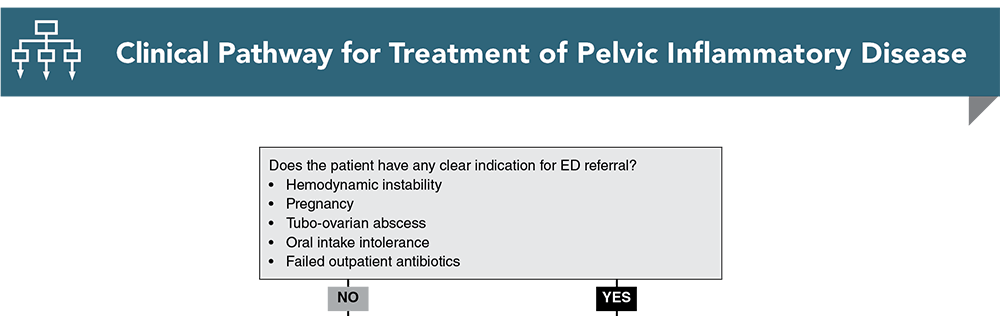
Subscribe to access the complete flowchart to guide your clinical decision making.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
11. * Workowski KA, Bachman LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1-180. (CDC guidelines) DOI: 10.15585/mmwr.rr7004a1
25. * Wiesenfeld HC, Meyn LA, Darville T, et al. A randomized controlled trial of ceftriaxone and doxycycline, with or without metronidazole, for the treatment of acute pelvic inflammatory disease. Clin Infect Dis. 2021;72(7):1181-1189. (Randomized double-blind placebo-controlled trial; 233 patients) DOI: 10.1093/cid/ciaa101
66. * Simms I, Warburton F, Weström L. Diagnosis of pelvic inflammatory disease: time for a rethink. Sex Transm Infect. 2003;79(6):491-494. (Retrospective; 623 patients) DOI: 10.1136/sti.79.6.491
90. * Tomas ME, Getman D, Donskey CJ, et al. Overdiagnosis of urinary tract infection and underdiagnosis of sexually transmitted infection in adult women presenting to an emergency department. J Clin Microbiol. 2015;53(8):2686-2692. (Prospective; 264 patients) DOI: 10.1128/JCM.00670-15
92. * Lee MH, Moon MH, Sung CK, et al. CT findings of acute pelvic inflammatory disease. Abdom Imaging. 2014;39(6):1350-1355. (Prospective; 231 patients) DOI: 10.1007/s00261-014-0158-1
96. Ross J, Cole M, Evans C, et al. United Kingdom national guideline for the management of pelvic inflammatory disease (2019 interim update).2019. (Guideline)
117. *Goyal M, Hersh A, Luan X, et al. National trends in pelvic inflammatory disease among adolescents in the emergency department. J Adolesc Health. 2013;53(2):249-252. (Retrospective NAHMCS database study) DOI: 10.1016/j.jadohealth.2013.03.016
135. *Marrazzo J. Molecular characterization of microbes in the female upper genital tract: a valiant quest to “redefine” pelvic inflammatory disease. J Infect Dis. 2021;224(12 Suppl 2):S36-S38. (Review) DOI: 10.1093/infdis/jiab301
136. *Mitchell C. To effectively treat pelvic inflammatory disease, look beyond coverage for gonorrhea and chlamydia. Clin Infect Dis. 2021;72(7):1190-1191. (Review) DOI: 10.1093/cid/ciaa103
Portions of this content were adapted from:
Taira T, Broussard N, Bugg C. Pelvic inflammatory disease: diagnosis and treatment in the emergency department. Emerg Med Pract. 2022;24(12):1-24. Used with permission of EB Medicine.
Subscribe to get the full list of 145 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: pelvic, cervical, uterus, adnexa, STI, endometritis, salpingitis, tubo-ovarian abscess, Fitz-Hugh-Curtis, ectopic, infertility, gonorrhea, chlamydia
Keith Pochick, MD
Margaret Carman, DNP, RN, ACNP-BC, ENP-BC, FAEN
Bradley Laymon, PA-C, CPC, CEMC
October 1, 2023
October 1, 2026 CME Information
4 AMA PRA Category 1 Credits™. 4 AOA Category 2-B Credits. Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 4 Infectious Disease CME credits and 1 Pharmacology CME credits
Evidence-Based Urgent Care • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Evidence-Based Urgent Care issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933