Table of Contents
-
Abstract
-
Case Presentation
-
Introduction
-
Critical Appraisal Of The Literature
-
Definition
-
Epidemiology
-
Pathophysiology
-
Differential Diagnosis
-
Neonates And Infants
-
Children
-
Prehospital Care
-
Emergency Department Evaluation
-
History
-
Physical Examination
-
Diagnostic Studies
-
Treatment
-
Special Circumstances
-
Disposition
-
Summary
-
Risk Management Pitfalls To Avoid In The Treatment Of Constipation
-
Case Conclusion
-
Clinical Pathway For The Treatment Of Constipation In Pediatric Patients
-
Tables and Figures
-
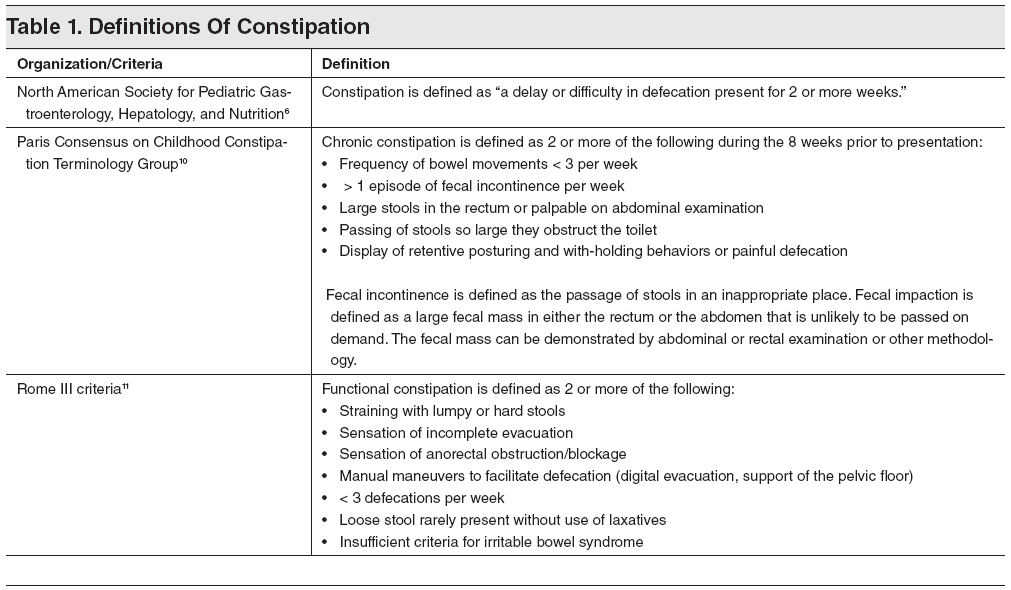
Table 1. Definitions Of Constipation
-
Table 2. Differential Diagnosis Of Constipation
-
Table 3. Medications For Use In The Treatment Of Constipation
-
Table 4. Treatment Recommendations For Constipation In Pediatric Patients
-
References
Abstract
A 1992 study showed that 7% of patients presenting to a pediatric emergency department (ED) with abdominal pain were diagnosed with constipation. Misdiagnosis of constipation may lead to multiple unresolved physician visits, utilization of emergency medical services, high doses of ionizing radiation, unnecessary laboratory tests, and even surgical procedures. This issue examines existing literature on constipation, though few randomized double-blind, controlled clinical trials of good quality existed in the literature until recently. The study populations in many articles are obtained from pediatric specialty clinics with subjects who carry a known diagnosis of chronic and often poorly controlled constipation. Analysis of the literature is hampered by lack of a concrete definition of constipation and the variability in outcome measures. The primary evidence-based recommendations are based on published guidelines and include management of constipation in children divided into 3 stages of therapy: (1) disimpaction, (2) maintenance therapy, and (3) behavior modification. Special consideration should be given to neonates and to children with pre-existing medical conditions.
Case Presentation
In the middle of a busy shift, you receive a call from a local general pediatrician who would like to transfer a 3-year-old boy whom she suspects has acute appendicitis. She describes the child as extremely uncomfortable, screaming, and grabbing his stomach in intense pain. She would like to have him evaluated by a pediatric surgeon as soon as possible. You accept the patient and agree that transporting the child by ambulance would be the most appropriate method of transfer. Upon arrival, the child is happy, playful, and in no obvious discomfort. This change in behavior is bewildering to his parents who explain to you that this is not the way the child looked earlier. Further history reveals that the child was in his usual state of good health until this morning when he suddenly began grabbing his belly and crying. He has had no fever, one episode of vomiting, which the mother relates to crying, and no stool changes. Your physical examination reveals a playful child who is running around the examination room, who is very well-appearing, and who laughs when you palpate his abdomen. The referring pediatrician has requested blood work, a CT scan, and a surgery consult. You do not want to expose this child to the unnecessary radiation of a CT, nor do you want to ignore the concern of the referring physician. What do you do next?
Introduction
Constipation is a seemingly benign condition that may be misunderstood as a simple and transient annoyance rather than a chronic condition. Misdiagnosis may lead to expensive, potentially harmful, and often unnecessary workups. Multiple unresolved physician visits, utilization of emergency medical services, high doses of ionizing radiation, unnecessary laboratory tests, and even surgical procedures may be ordered and performed when a simple digital rectal examination or an abdominal radiograph would have provided the diagnosis.1
Alternatively, some children who are appropriately diagnosed with constipation are not treated aggressively enough, parents are not fully educated about the condition and its management, and the diagnosis may be minimized by both the provider and caregiver. One longitudinal study of constipated children found that 30% of subjects continued with complaints into young adulthood, and half of them experienced at least 1 relapse within 5 years of initially successful treatment.2
Lack of a concrete definition of constipation, great variability in the management of this condition, and lack of evidence-based treatment recommendations further complicate the diagnosis and treatment of constipation. Successful management of the constipated pediatric patient depends on accurate diagnosis, appropriate initial and maintenance therapy, detailed parental education, and consistent follow-up.3 The emergency clinician is often the first to make the diagnosis of constipation, plan initial therapy, make appropriate subspecialty referrals, and prevent unnecessary and wasteful evaluations.
Critical Appraisal Of The Literature
To date, much of the evaluation and management of constipation in children is based on opinion, authority, and personal preference rather than evidence. There have been few randomized double-blind controlled clinical trials of good quality in the literature until recently. Furthermore, it is difficult to perform a systemic analysis of the literature because of the lack of a concrete definition of constipation and the variability in outcome measures (ie, definition of treatment success). The study populations in many of these articles are obtained from pediatric specialty clinics with subjects who carry a known diagnosis of chronic and often poorly controlled constipation.
Pijpers et al searched the MEDLINE® and Embase databases for all studies on constipation in children published before December 2007. The researchers assessed the quality of the resulting studies using the Delphi list, a validated quality score tool. They found that only 10 studies were of high quality and concluded that there is no evidence to support the use of one particular method of treatment of constipation over another.4
The author’s search resulted in 33 pertinent references for this article. Of the limited number of quality studies available, even fewer pertain to diagnosis and management in the pediatric ED.
Risk Management Pitfalls To Avoid In The Treatment Of Constipation
-
“Babies and children who do not stool every day are constipated.” Stool pattern among infants and children is highly variable, and the number of bowel movements generally decrease as age increases. Neonates and infants will often grunt and strain as they defecate. This behavior is normal as they learn the process of coordinating their internal and external sphincters. Parental education about normal and abnormal stool patterns is important to help identify children who need therapy and to avoid unnecessary physician visits.
-
“My child has normal bowel movements every day, so there is no way he can be constipated.” Children with crampy, episodic, and often severe abdominal pain will frequently present without any history of hard or infrequent stool. Parents are often surprised or may even doubt that such a seemingly benign diagnosis could be capable of causing such pain. Further, children often undergo extensive and often unnecessary laboratory and radiological evaluations when a plain abdominal radiograph would have revealed moderate or even severe fecal retention.
-
“I do not feel a fecal mass on abdominal examination or digital rectal examination, so a fecal impaction is unlikely.” The presence of a fecal mass on abdominal or rectal examination is indeed helpful if it is present. Many constipated children and even those with a fecal impaction will have normal abdominal and rectal examinations. In this case, a plain abdominal radiograph is helpful in identifying the presence and extent of fecal loading.
-
“There is no way my child can be constipated. He is having diarrhea and vomiting.” Encopresis, or overflow diarrhea, is a result of a combination of factors. A large fecal mass, chronic stretching of the colon, loss of colonic sensation, and propulsive force all work to allow softer, proximal stool to leak around a large stool mass. The presence of vomiting (in this case) mimics acute gastroenteritis. The absence of fever, sick contacts, and the presence of moderate to severe abdominal pain with or without a prior history of constipation should alert the clinician to the possibility of encopresis.
-
“A fecal impaction must be cleared with an enema.” The initiation of the removal of a fecal impaction is important in the ED, especially if the cause of abdominal pain is uncertain and the clinician needs to assess response to removal of the fecal mass. In this case, enemas are usually fast and effective. In the child who is otherwise stable, has a benign abdominal examination, and lacks red flags that would point to an organic cause of constipation, disimpaction can be performed with either enemas or oral polyethylene glycol. An individualized approach is reasonable in this case. Patients who use enemas are likely to have transient abdominal pain. Patients using oral polyethylene glycol are likely to have episodes of incontinence.
Tables and Figures
References
Evidence-based medicine requires a critical appraisal of the literature based upon study methodology and number of subjects. Not all references are equally robust. The findings of a large, prospective, randomized, and blinded trial should carry more weight than a case report.
To help the reader judge the strength of each reference, pertinent information about the study, such as the type of study and the number of patients in the study, will be included in bold type following the reference, where available. In addition, the most informative references cited in this paper, as determined by the authors, will be noted by an asterisk (*) next to the number of the reference.*
-
Diamanti A, Bracci F, Reale A, et al. Incidence, clinical presentation, and management of constipation in a pediatric ED. Am J Emer Med. 2010;28:189-194. (Retrospective study; 202 subjects)
-
* Liem O, Harman J, Benninga M, et al. Health utilization and cost impact of childhood constipation in the United States. J Pediatr. 2009;154:258-262. (Database review; 21,778 subjects)
-
Pijpers MA, Bongers ME, Benninga MA, et al. Functional constipation in children: a systematic review on prognosis and predictive factors. J Pediatr Gastroenterol Nutr. 2010;50:256-258. (Review article)
-
* Pijpers MA, Tabbers MM, Benninga MA, et al. Currently recommended treatments of childhood constipation are not evidence based: a systematic literature review on the effect of laxative treatment and dietary measures. Arch Dis Child. 2009;94:117-131. (Review article)
-
* van den Berg MM, Benninga MA, DiLorenzo C. Epidemiology of childhood constipation: a systematic review. Am J Gastroenterol. 2006;101:2401-2409. (Review article)
-
* Constipation Committee of the North American Society for Pediatric Gastroenterology, Hepatology, And Nutrition. Evaluation and treatment of constipation in children: recommendations of the north american society for pediatric gastroenterology, hepatology, and nutrition. J Pediatr Gastroenterol Nutr. 2006;43:e1-e13. (Review article)
-
* Pirie J. Management of constipation in the emergency department. Clin Pediatr Emerg Med. 2010;11:182-188. (Review article)
-
Iacono G, Francesca C, Montalto G, et al. Intolerance of cow’s milk and chronic constipation in children. N Engl J Med. 1998;339:1100-1114. (Double-blind crossover study; 65 subjects)
-
* Bekkali NL, van den Berg MM, Dijkgraaf MG, et al. Rectal fecal impaction treatment in childhood constipation: enemas versus high doses oral PEG. Pediatrics. 2009;124:e1108-1115. (Randomized controlled trial; 90 subjects)
-
Benninga M, Candy DC, Catto-Smith AG, et al. The Paris Consensus on Childhood Constipation Terminology (PACCT) Group. J Pediatr Gastroenterol Nutr. 2005;40:273-275. (Consensus definition)
-
Longstreth GF, Thompson WG, Chey WD, et al. Functional Bowel Disorders. Gastroenterology. 2006;130:1480-1491. (Consensus definition)
-
Clayden G, Wright A. Constipation and incontinence in childhood: two sides of the same coin? Arch Dis Child. 2007;92:472-474. (Review article)
-
Culbert TP, Banez GA. Integrative approaches to childhood constipation and encopresis. Pediatr Clin N Am. 2007;54:927-947, xi. (Review article)
-
Rockney RM, McQuade WH, Days AL. The plain abdominal roentgenogram in the management of encopresis. Arch Pediatr Adolesc Med. 1995;149:623-627. (Retrospective case study; 60 subjects)
-
Loening-Baucke V. Prevalence rates for constipation and faecal urinary incontinence. Arch Dis Child. 2007;92:486-489. (Retrospective review; 482 subjects)
-
Bardisa-Ezcurra L, Ullman R, Gordon J, et al. Diagnosis and management of idiopathic childhood constipation: summary of NICE guidance. BMJ. 2010;340:c2585. (Review article)
-
Focht DR 3rd, Baker RC, Heubi JE, et al. Variability in the management of childhood constipation. Clin Pediatr. 2006;45:251-256. (Cross sectional survey)
-
Loening-Baucke V, Swidsinski A. Constipation as a cause of acute abdominal pain in children. J Pediatr. 2007;151:666-669. (Chart review; 1002 children)
-
* Biggs WS, Dery WH. Evaluation and treatment of constipation in infants and children. Am Fam Physician. 2006;73:469-477. (Review article)
-
Rahman Z, Gerayli F, Carter NJ. What treatment works best for constipation in children? J Fam Pract. 2009:58:329-331. (Review article)
-
* Bulloch B, Tenenbein M. Constipation: diagnosis and management in the pediatric emergency department. Pediatr Emerg Care. 2002;18:254-258. (Review article)
-
Miller MK, Dowd MD, Franker M. Emergency department management and short-term outcome of children with constipation. Pediatr Emerg Care. 2009;58:329-331. (Chart review; 121 subjects)
-
Bongers ME, van den Berg MM, Reitsma JB, et al. A randomized controlled trial of enemas in combination with oral laxative therapy for children with chronic constipation. Clin Gastroenterol Hepatol. 2009;7:1069-1074. (Randomized controlled trial; 102 subjects)
-
Kokke F, Scholtens P, Alles MS, et al. A dietary fiber mixture versus lactulose in the treatment of childhood constipation: a double-blind randomized control trial. J Pediatr Gastroenterol Nutr. 2008:47:592-597. (Double-blind randomized controlled trial; 135 subjects)
-
Candy D, Belsey J. Macrogol (polyethylene glycol) laxatives in children with functional constipation and fecal impaction: a systematic review. Arch Dis Child 2009;94:156-160. (Review article)
-
Thomson MA, Jenkins HR, Bisset WM, et al. Polyethylene glycol 3350 plus electrolytes for chronic constipation in children: a double blind, placebo controlled, crossover study. Arch Dis Child. 2007;92:996-1000. (Double blind controlled crossover study; 51 subjects)
-
Nurko S, Youssef N, Sabri N, et al. PEG3350 in the treatment of childhood constipation: a multicenter, double-blinded, placebo-controlled trial. J Pediatr. 2008;153:254-261. (Prospective randomized multicenter double-blind placebo controlled study; 103 subjects)
-
* Pasbankar DS, Bishop WP. Efficacy and optimal dose of daily polyethylene glycol 3350 for treatment of constipation and encopresis in children. J Pediatr. 2001;139:428-432. (Prospective study; 20 subjects)
-
Chung S, Cheng A, Goldman R. Polyethylene glycol 3350 without electrolytes for treatment of childhood constipation. Canad Fam Physician. 2009;55:481-482. (Review article)
-
* Youssef NN, Peters JM, Henderson W, et al. Dose response of PEG 3350 for the treatment of childhood fecal impaction. J Pediatr. 2002;141:410-414. (Prospective double-blind parallel randomized study; 40 subjects)
-
Harrington L, Schuh S. Complications of fleet enema administration and suggested guidelines for use in the pediatric emergency department. Pediatr Emerg Care. 1997;13:225-226. (Review article)
-
* Candy DC, Edwards D, Geraint M. Treatment of faecal impaction with polyethylene glycol plus electrolytes (PGE+E) followed by a double-blind comparison of PEG+E versus lactulose as maintenance therapy. J Pediatr Gastroenterol Nutr. 2006;43:65-70.(Randomized double-blind comparison study; 65 subjects)
-
33. Corkins MR. Are diet and constipation related in children? Nutr Clin Prac. 2005;20:536-539. (Review article)








 678-366-7933
678-366-7933