

Another study reviewed 371 cases of children presenting to the pediatric ED with abdominal pain.3 Gastroenteritis and nonspecific abdominal pain accounted for nearly 60% of cases. Respiratory tract illnesses, including pharyngitis, asthma, otitis, and pneumonia, were diagnosed in 12% of patients. Surgical causes, including appendicitis, bowel obstruction, abdominal trauma, intussusception, strangulated hernia, cholelithiasis, and malrotation, accounted for 6.5% of cases. Appendicitis—comprising about 3% of the series—was the only surgical diagnosis to occur more than 1% of the time.
These studies indicate that abdominal pain in children is secondary to diverse etiologies, but that surgery is rarely necessary (0.05% of all visits, 1%-3% of visits for abdominal pain).
A comprehensive differential diagnosis of abdominal pain in children of all ages4 can be soporific even for the insomniac. In this section we discuss a short list of critical diagnoses that should be considered. A comprehensive list is so ponderous as to be practically useless for an ED evaluation.
The diagnoses of most concern are those that require operative intervention. The three most common surgical conditions are appendicitis, incarcerated inguinal hernia, and intussusception.7
When developing a differential diagnosis, consider the child's age. For example, intussusception is most commonly seen in children between 4 and 10 months of age5,6 but almost never in adolescents. (See Table 2.)

Although appendicitis occurs in nearly all age groups, the incidence peaks in older school-age children.8 The classic presentation consists of constant, vague periumbilical pain followed by vomiting, migration of the pain to the right lower quadrant, and low-grade fever.9 Table 3 presents features that Wagner suggests best identify appendicitis.

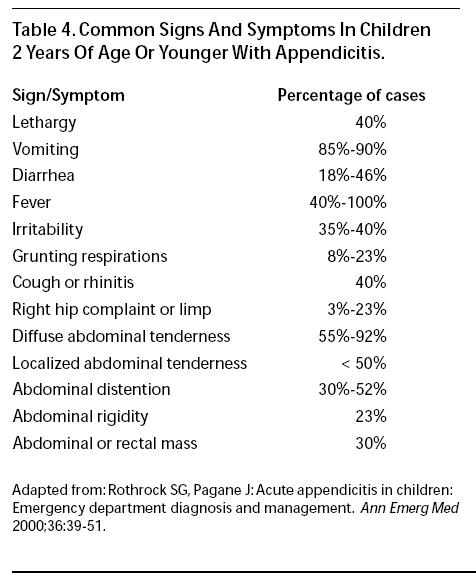
Unfortunately, young children are poor historians and localize abdominal pain poorly. This may be responsible for the fact that as many as 60%-100% of toddlers will perforate by the time they are diagnosed. 10,11 In one study of 120 children 5 years of age or younger, more than 40% of the patients had a delayed diagnosis while nonsurgical diagnoses were explored.11 Children 2 years of age or younger with appendicitis commonly have symptoms or signs, including cough, rhinitis, grunting respirations, and walking with a limp, that lead the emergency physician or pediatrician away from the correct diagnosis.12 (See Table 4.)
The most common misdiagnoses in cases of appendicitis in children include gastroenteritis (42%) and a variety of upper respiratory tract infections (18%).13 The presence of diarrhea can be particularly misleading; diarrhea occurs in up to one-third of children under the age of 3 years with appendicitis.14

The incidence of inguinal hernia is greatest during early infancy; boys are affected six times more often than girls.15 Unlike umbilical hernias, inguinal hernias generally do not resolve but instead become incarcerated or strangulated 12-20% of the time.16,17 Infants with incarcerated hernias typically have crampy abdominal pain, vomiting, and irritability. The emesis may become bilious as the obstruction persists.7 While the overlying skin is usually normal, it may become erythematous or purple as the condition progresses.8
Intussusception is another condition that typically strikes infants. Affected children are usually between the ages of 2 months and 5 years (with a peak incidence between 4 and 10 months of age).5,6 The classic triad consists of colicky intermittent abdominal pain, vomiting, and bloody stool. However, this constellation is seen in only 10%-20% of documented cases.18 Currant jelly stools occur even less frequently.19 More commonly, infants have periods of crying and drawing up their legs followed by periods of appearing playful and normal. A right upper-quadrant mass may be palpable. This is because the site of the telescoping bowel is usually at the ileocecal junction.5,6 The diagnosis of intussusception may be obscured if the patient presents with nonspecific symptoms, including lethargy, pallor, or shock.6 A subset of infants with intussusception present with suspected sepsis or central nervous system dysfunction, including generalized weakness, lethargy, and even seizures.20 The connection between intussusception and neurologic symptoms is not well-understood but is thought to be due to neurochemical mediators.20 When this is the case, coming to the correct diagnosis can be extremely difficult, particularly if bloody stool is not found on rectal exam or if a rectal exam is not performed. In one study, 75% of children with intussusception tested positive for occult blood in the stool.21
Although testicular torsion typically presents with scrotal discomfort, some children localize the pain to their abdomen.5,22 While testicular torsion can be seen at any age, there is a bimodal age distribution. A small peak occurs in the neonatal period, but cases predominate in older school-age children and young adolescents. 23-26 Many of the neonatal cases involve torsion that occurs before birth. The swollen, discolored scrotum is identified in the nursery, and the testis is not viable by that time.
Malrotation with midgut volvulus is a true surgical emergency. Although symptomatic malrotation may occur in children older than 1 year of age, the vast majority of cases occur in the neonate. In older children, the time course of the symptoms is usually measured in months.
Malrotation is characterized by intermittent vomiting and abdominal pain.27 In neonates, bilious vomiting is considered a hallmark of the condition. In one series, bilious vomiting was present in all infants with midgut volvulus.27
Unfortunately, child abuse or non-accidental trauma (NAT) is always a possible cause of abdominal pain. Clues to abuse include bruises of varying ages, ecchymoses in unusual locations, untreated burns, and fractures in varying stages of healing. Parents may give inconsistent stories for these findings. In addition to solid organ injury, NAT may involve the gut. A sharp blow to the upper abdomen can produce a duodenal hematoma. This results in obstruction and relentless vomiting, absent any external signs of trauma.
Although not typically considered a disease of childhood, ectopic pregnancy must be considered in preteen and teenage girls. Their denials of sexual contact may be unreliable, particularly when a parent is present during the history taking. A significant percentage of females who deny sexual activity may be pregnant.28 A pregnancy test should be performed on menstruating females with abdominal pain, regardless of age.
Other gynecologic conditions occur in school-age and adolescent girls. Ovarian torsion typically presents as moderately severe lower abdominal pain, localized to one side. When the right ovary is torsed, differentiating this diagnosis from appendicitis may require laparoscopy, laparotomy, or computerized tomography. 29 The rupture of a hemorrhagic cyst can present in a dramatic fashion, with hypotension, abdominal tenderness, and referred shoulder pain (from blood irritating the diaphragm). A negative pregnancy test in this case does not preclude emergent laparotomy. In addition, pelvic inflammatory disease with or without peritonitis may present in sexually active teens. It also occurs in preadolescent victims of sexual abuse.
The presentation of urinary tract infections (UTIs) often depends on the age of the child. Neonates with UTIs may be febrile and appear septic. In addition to fever, infants with UTI can have vomiting and diarrhea. 30 Also, consider UTI if a previously toilet-trained child begins wetting her pants. UTIs in preschool and school-age girls are usually associated with gastrointestinal complaints, including abdominal pain and vomiting without diarrhea. In adolescent girls, urinary tract infections mimic the adult pattern of dysuria, urinary frequency, and urinary urgency.
A simple clean-catch urinalysis is essential in toilet-trained young girls with abdominal pain. However, the finding of white cells in the urine does not clinch the diagnosis, as some cases of appendicitis also present with low-grade pyuria (and even bacteruria).31,32
Nonsurgical causes of abdominal pain range from the pathologically inert (e.g., school anxiety) to the lifethreatening. Strep pharyngitis is a common cause of abdominal pain in school-age children and is responsible for up to 16% of cases.2 Diabetic ketoacidosis causes dramatic abdominal pain and vomiting. Absent a history of diabetes, the fruity odor of ketones and a recent history of polyuria and polydipsia will suggest the diagnosis. Lobar pneumonia is another important cause of abdominal pain. While cough and fever are typically present, these may be overshadowed by the abdominal complaints. Other unusual "extra-abdominal" causes of abdominal pain include the bites of scorpions and black widow spiders, poisoning from lead or other heavy metals, porphyria, and Rocky Mountain spotted fever.33
Constipation can cause abdominal pain. While some physicians obtain an x-ray to evaluate a child for constipation, this is not supported by the literature.34,35 The presence of stool on plain radiographs does not exclude alternative diagnoses. Infants, particularly some breast-fed infants, may stool only once in several days. When parents ask to have their child evaluated for "constipation," ascertain good weight gain, a wellappearing infant, and a history of soft stools. Reassurance and follow-up with their primary doctor may be all that are required.
Gastroenteritis is one of the most common causes of abdominal pain in children. The crampy pain may result from the increased intestinal motility, or children may interpret their nausea and malaise as "abdominal pain." These children typically have both vomiting and diarrhea, often accompanied by fever. Their abdomens are typically soft and nontender and demonstrate increased bowel sounds. Vomiting and diarrhea are also commonly seen in appendicitis (see Table 4), and failure to perform an adequate initial or repeat examination risks missed pathology.10-14,36,37 Serial examinations in the ED can help distinguish gastroenteritis from other, more serious etiologies. The moderately dehydrated child with gastroenteritis will often dramatically improve after oral or intravenous hydration.
Infant colic is a controversial diagnosis.38-40 Concerned parents may present with a child who has cried for the greater part of an evening, apparently from abdominal pain. Typically, these infants are younger than 4 months of age. (A full discussion of the inconsolable infant is beyond the scope of this article; a good source is: Pawel BB, Henretig FM: Crying and colic in early infancy. In: Fleisher GR, Ludwig S, Henretig FM, eds. Textbook of Pediatric Emergency Medicine. Philadelphia: Williams & Wilkins; 2000:193-195.)
Unfortunately, there are other features that are common to many clinical entities. These include vomiting, diarrhea, fussiness or irritability, vague complaints of diffuse pain, and fever. Parents are likely to mislead the emergency physician in cases of nonaccidental trauma.
Determine the chronicity of the pain. Children with recurring and persistent abdominal pain may have had multiple medical investigations in the past. In the absence of organic disease, chronic pain (especially only occurring on weekdays) may be associated with stress, school anxiety, or even parental illness or neurosis.41 Chronic Recurring Abdominal Pain is sometimes referred to by its unfair (and scatological) acronym.
The abdominal examination in the young child requires artistry. While palpating the abdomen of a preschooler, asking "Does this hurt?" always gets an affirmative nod to every location touched. Frustrated parents frequently say, "Tell the doctor where it hurts"—to little avail. Likewise, forcing a kicking and screaming young child onto the gurney and then trying to palpate his or her abdomen is similarly fruitless.
Several approaches to the examination of the pediatric belly have been described; unfortunately, there is essentially no data available to validate them. That said, here are some of our favorite techniques.
When examining neonates and young infants, flex their knees to their abdomen, as this will soften their abdominal muscles. Allow the fearful child to remain seated in the parent's lap during abdominal palpation. Watch their facial expressions instead of asking for verbal affirmations of pain.
Another strategy is making the examination a game. A child with a tender abdomen will play until a sensitive area is examined. Tell them that you are going to feel their belly to guess what they ate; having them participate can promote a better exam. Palpating for gummy worms and toast is sure to reassure the child of your professionalism. Some physicians pretend to blow out imaginary candles on the child's abdomen.
If the abdomen is tender, assess for peritoneal signs. An alternative to rebound testing is to have the child jump up and down. Children with appendicitis typically jump only once, as the painful landing abruptly terminates the game.
A hurried physical exam without complete exposure will miss an inguinal hernia or testicular torsion. In the young child, "dropping the diaper" is an essential maneuver. Simply undressing the child may yield a prompt diagnosis. Feel for an incarcerated inguinal hernia and look for the scrotal discoloration while palpating for an abnormal testicular lie. A grossly bloody stool in the diaper of a lethargic child points to intussusception.
The value of a rectal examination in children with abdominal pain is controversial. On the one hand, localized tenderness, fecal impaction, or heme-positive stools can be important findings. On the other hand, a review of its clinical utility shows that it is rarelyhelpful.45 In one study of 1140 children 2-12 years old with acute abdominal pain, the authors noted that of eight patients with appendicitis in whom a rectal examination was performed, findings were noncontributory in six.46 Overall, they believed that the rectal examination was clinically useful in 12 of 56 patients (21%): five with constipation, three with gastroenteritis, two with appendicitis, and one patient each with abdominal adhesions and abdominal pain of uncertain etiology.
Although there is no literature directly supporting this practice, per se, we recommend a pelvic examination be performed on all sexually active teen females with abdominal pain. Prominent cervical motion tenderness or an adnexal mass may lead the emergency physician to the correct diagnosis. In the virginal preteen or teenage female with abdominal pain, the preferred approach is the bimanual rectal examination. In this exam, the examiner does not place anything in the vagina. Instead, the examiner palpates the uterus and adnexa via a finger in the rectum. In this manner large masses or prominent tenderness may be appreciated.
There are only a few diagnostic studies that are helpful when evaluating a child who complains of abdominal pain. The history and physical examination are typically the most powerful tools available to the emergency physician. However, diagnostic studies have come to play a prominent role in many cases of vague abdominal pain, particularly when accompanied by abdominal tenderness.
Despite its ubiquity, the complete blood count (CBC) is rarely helpful in the management of children with acute abdominal pain. While inexpensive and commonly used, this fact is inescapable: Leukocytosis in young children is profoundly nonspecific andfairly insensitive.47 Children with gastroenteritis may have a high white count with a left shift,48,49 while as many as 40% of those with appendicitis may have no leukocytosis.50
There are no good studies that evaluate the utility of the CBC in developing either a diagnosis or management plan for children with abdominal pain. A single study looked at the white blood cell (WBC) count and appendicitis in a blinded fashion in adults 15-45 years of age with suspected appendicitis.51 The average total WBC count was statistically significant between patients found to have appendicitis (12.6 x 106/L) and those found not to have appendicitis (8.9 x 106/L). However, it is not at all clear that these two WBC counts are clinically different, as the ranges of WBC counts in the two groups were nearly the same (4.9- 22.2 x 106/L in those with appendicitis and 4.2-17.7 x 106/L in those without appendicitis). Looking at the WBC count greater than 15.0 x 106/L, there was 93% specificity for appendicitis, but only 29% sensitivity. Using decision analysis on this data, there is less than a 20% chance that a WBC count will appropriately affect clinical decision making in patients with possible appendicitis.52
In summary, the CBC cannot be considered a standard of care in the routine evaluation of children with abdominal pain. In one large ED study of children with acute abdominal pain, it was ordered only 8% of the time.53 This said, an emergency physician should not be surprised if he or she is asked about the white count when consulting a surgeon regarding a child with abdominal pain.
In one large study of children with abdominal pain, chemistry studies were ordered about 4% of the time.53 Tests included electrolytes, blood urea nitrogen, glucose, creatinine, calcium, phosphorus, uric acid, cholesterol, total protein, albumin, bilirubin, alkaline phosphatase, and serum glutamic oxaloacetic transaminase (SGOT). In this study, these values were normal about 75% of the time. The abnormalities primarily reflected dehydration or hepatitis. In general, aside from diagnosing concomitant dehydration, little diagnostic information is gained from a set of electrolytes.
A urinalysis is inexpensive and can identify UTIs. An important caveat is that an inflamed appendix adjacent to the bladder can result in pyuria. One study included 50 children 2-16 years old with surgically confirmed appendicitis. Nine of these 50 children (18%) had pyuria (defined as greater than 4 WBC per high power field).31 In another study, 194 consecutive school-age children 7-15 years old who underwent appendectomy had a urinalysis performed. Thirteen of the 156 patients (8%) who had appendicitis had abnormal urinalyses.32
A dipstick urinalysis is also valuable to evaluate for ketosis and hyperglycemia. In a child with abdominal pain, a normal dipstick urine should rule out diabetic ketoacidosis (DKA). Even if the glucose part of the strip is not considered, the dipstick test for ketones is 97% sensitive for DKA.54
Hypoglycemia is occasionally seen in children with vomiting and diarrhea.55 A bedside glucose is inexpensive and will promptly identify glucose abnormalities. It is essential in the child with altered mental status. Bedside glucose testing is also valuable in patients suspected of DKA.
Most experienced emergency physicians and pediatric surgeons will admit to having been fooled by pneumonia- associated abdominal pain. (The ones who do not admit this are either neophytes or disingenuous.) Pneumonia may be the culprit even if coughing is not the predominant complaint. In one large study, 2.3% of children with abdominal pain had a final diagnosis of pneumonia.2 Some indications for a chest film in the febrile child with abdominal pain include:56
Plain radiographs of the abdomen are rarely helpful in evaluating children with abdominal pain. Their value is limited to clinical scenarios where a physician suspects perforation, obstruction, or midgut volvulus. While there are other findings that are occasionally helpful (see Table 5), free air, multiple air fluid levels, and the "double bubble" sign are the "big three." Most plain films of the abdomen provide little useful information. Many emergency physicians may recognize this fact, as in some centers these x-rays are infrequently ordered. In one study of more than 1100 children with abdominal pain, abdominal films were ordered only 3.5% of the time.53
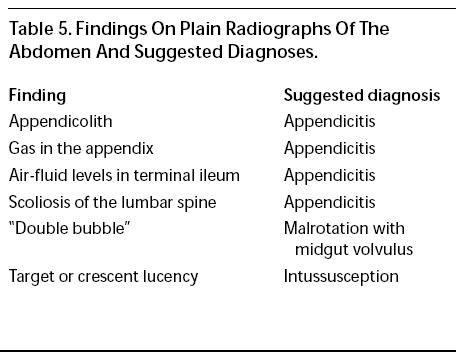
In evaluating a neonate or young infant with bilious vomiting, the emergency physician may order abdominal x-rays to look for a "double bubble" sign. This sign of midgut volvulus occurs when air in the stomach and air in the adjacent obstructed duodenumappear as adjacent bubbles. Although highly specific, the double bubble is rare.57 It also occurs with duodenal atresia, which is usually picked up immediately after birth.
Plain films should not be routine in the evaluation of suspected appendicitis. Occasionally, an appendicolith may be visualized on plain film. (See Table 5.) Unfortunately, specific findings (some of which are quite subtle) are seen in as few as 24% of patients with appendicitis and as many as 60% of patients without appendicitis.58 In one study involving cases of suspected appendicitis, 79% of abdominal x-rays were normal.35 In a more recent study, the cost involved in making a correct diagnosis based on plain film was $1593, compared to $270 for computed tomography.59
When considering intussusception, some physicians obtain plain abdominal x-rays before ordering additional imaging studies (i.e., ultrasound or barium/ air enema). Unfortunately, plain radiographs are neither sensitive nor specific enough to rule in or rule out intussusception.60
Air and barium enemas are very useful in the child with suspected intussusception. Air has several advantages over barium in that it is relatively inert and causes fewer problems if a perforation occurs during reduction attempts.
Enemas have their downside. An enema can perforate the bowel if the gut is ischemic. If a perforation does occur, barium can cause peritonitis. Gastrografin has a high osmolality and can produce shock (secondary to intravascular depletion) in the case of perforation.
For these reasons, some centers prefer air contrast enemas since they result in smaller tears in the event of perforation. Using air is less expensive, requires less radiation, and leads to shorter fluoroscopy times.61 Success rates are similar with the two modalities.61-63 However, air is a poor contrast medium, so lead point masses can be missed. In addition, if an intestinal mass causes an intussusception, surgical repair is favored over hydrostatic reduction.
The use of ultrasound to evaluate children with abdominal complaints has gained favor in the past decade. Ultrasound can provide important information regarding pyloric stenosis, intussusception, appendicitis, abdominal masses, testicular torsion, and gynecologic disorders.64
There are several advantages to ultrasound in children. It is safe and noninvasive and can be performed on non-sedated young children. In addition, ultrasound can be employed at the bedside of unstable patients. It performs well in children, who generally have small abdomens with minimal fat.
On the other hand, ultrasound is very operatordependent and requires considerable experience to obtain adequate images, particularly when used to evaluate for appendicitis.57,64,65 In one study, a single radiologist had a sensitivity of 0% for appendicitis65 (adding new meaning to the term "blinded radiologist"). Smaller facilities and those that lack experience in pediatric ultrasounds may be equally frustrated by this modality.
When evaluating a child for intussusception, the air or barium study is the traditional gold standard. However, ultrasound is now used with growing frequency. One recent study showed it had a sensitivity of 93% and a specificity of 98% in experienced hands.18 In another trial, ultrasound detected all cases of intussusception. 64 For this reason, some facilities perform an ultrasound as the initial test for intussusception. (However, other centers believe that because the enema studies can be both diagnostic and therapeutic, ultrasound interposes an unnecessary step.)
Color-flow Doppler ultrasound can also identify areas of infarcted bowel. Normal blood flow on Doppler indicates that ischemia is unlikely and thus reduces the risk of perforation during a therapeutic enema.
When intussusception is identified by ultrasound, it may be followed by a barium enema, which can reduce the intussuscepted bowel. If the ultrasound identifies a mass at the leading edge, the enema is superfluous and the child may proceed to surgery.
When the diagnosis is not obvious from clinical signs and plain films ("double bubble" sign), an upper GI series is the traditional gold standard for the diagnosis of midgut volvulus. However, ultrasound may also suggest the diagnosis. The most telling finding is the presence of the superior mesenteric artery on the right side of the superior mesenteric vein instead of in its normal position on the left. A normal ultrasound cannot rule out midgut volvulus, as the relationship of the mesenteric vessels may be normal in as many as one-third of surgically proven cases of midgut volvulus.57
Intravenous pyelography (IVP) was the time-honored study of choice in adults and children with suspected renal colic. However, ultrasound can reveal either stones or hydronephrosis without the use of ionizing radiation or contrast media. Stones in the medullary pyramids and collecting system of the kidney are best seen in young infants, as renal fat in older children fogs the sonographic windows. An obstructing or partially obstructing stone in the distal ureter will produce dilatation of the ureter apparent on ultrasound; sometimes even the calculus can be identified. However, in the absence of these findings, ultrasound may falsely negative.64
Ultrasound is used in many centers to evaluate children for appendicitis.57 The sensitivity and specificity are generally good but can vary widely. In three recent pediatric studies, the sensitivity ranged from 82% to 94%, and the specificity ranged from 89% to 100%.66-68 While a positive ultrasound is helpful in making the diagnosis, ultrasound is poor at excluding appendicitis.65,69-71 Because of this, some hospitals routinely obtain a limited abdominal CT if the ultra-sound is negative or equivocal.71,72
In general, ultrasound is best suited for children with an intermediate suspicion for appendicitis. Ultrasound is unnecessary when clinical suspicion is high, as such patients require laparotomy. However, when the clinical picture is less clear, ultrasound may improve diagnostic accuracy.73
Although an increasing number of studies have examined the role CT in adults with abdominal pain,74,75 these studies have included few children. The youngest children in these studies are 6 and 8 years of age. However, the use of CT scanning in adults appears promising, with sensitivities ranging from 96% to 100% and specificities from 95% to 99%.74,75 Two studies have looked at the use of limited CT scans using only rectal contrast or no contrast at all.71,72
One interesting approach is to combine ultrasound and CT as sequential studies. One trial evaluated 139 children 3 to 21 years old (mean, 11 years) with equivocal clinical findings for acute appendicitis.71 Utilizing ultrasound as the initial test, patients underwent laparotomy if the ultrasound was definitive for appendicitis. If the ultrasound was negative or inconclusive, a CT scan was then performed (utilizing rectal contrast without oral or intravenous contrast). This protocol resulted in a sensitivity of 94% and specificity of 94% for acute appendicitis in those children who underwent both studies. The subsequent CT scan was an important diagnostic safeguard, since the ultrasound examination was 93% specific but only 44% sensitive.
While many of the studies from the mid-1990s employed rectal contrast, recent data suggests that unenhanced CT is highly accurate in the diagnosis of appendicitis (97% accurate).75 The unenhanced study is performed without the oral, intravenous, or rectal contrast. Further work will need to be done to evaluate the utility of unenhanced CT in children.
Helical CT scanning for renal colic does not require an IV or IV contrast administration. Unenhanced helical CT is more sensitive for renal and ureteral calculi than IVP.64,76 The CT can demonstrate signs of a recently passed stone, such as perinephric or periureteral fat stranding, ureteral wall edema, ureteral dilatation, and blurring of renal sinus fat.77 In addition, it can elucidate other causes of flank pain.76
when he's not examining me,
is home studying medicine."
—George S. Kaufman (1889-1961)
Appendicitis and mesenteric occlusion share similar physical findings. Although the data is limited, it has been suggested that the incidence of appendicitis in children with sickle cell disease is lower than that in the general pediatric population.79,80 However, based on a small series (9 patients), appendicitis may have a more rapid course and a higher incidence of perforation (66%) in patients with sickle cell disease.79
Patients with sickle cell disease may also demonstrate a "right upper quadrant syndrome" related to a multitude of problems affecting the liver or gallbladder. The patient may present with acute pain, right upper-quadrant tenderness, and jaundice. Again, leukocytosis is common and nonspecific. Etiologies include hepatic abscess, cholelithiasis, cholecystitis, and hepatic infarcts.4,78 CT scanning and right upperquadrant ultrasound are useful imaging modalities.
Medication side effects may also muddy the diagnostic waters in these complex kids. For instance, certain antiviral agents can cause severe or even fatal pancreatitis.81
Such children may also harbor significant pathology despite a relatively benign examination and normal diagnostic tests. The following case illustrates this diagnostic hurdle: A technology-dependent child presented to the ED for the evaluation of abdominal pain. The child had an equivocal exam, an indeterminate ultrasound, and an abdominal CT scan that was technically limited. The child was then admitted for observation, improved over the next 24 hours, and was discharged home. The patient returned three days later with perforated appendicitis.71

Several other factors influence decision-making. In general, the abdominal pain must resolve in order for the child to be considered for discharge home. An exception may be those children with an obvious cause for their pain (such as exudative pharyngitis or pneumonia). In most circumstances, prolonged observation or admission and consultation are preferable to sending a child home with ongoing pain.
Also, consider the home circumstances. Remote locations, absence of a phone or transportation, or an unstable home situation may require prolonged observation or admission. The possibility of child abuse should be excluded.
Follow-up will vary depending upon local practice.
Some physicians working in certain academic centers may arrange follow-up with a pediatric surgeon. For most communities, the family practitioner or pediatrician will provide later care. In medically underserved areas (including the inner city), the ED may deliver the most reliable follow-up.
In general, the rules are as follows:
missed the diagnosis of appendicitis, and those who are
going to miss the diagnosis of appendicitis."
Scoring systems such as the MANTRELS or Alvarado score may improve diagnostic accuracy in adults with suspected appendicitis. However, the available literature suggests that such systems do not aid diagnosis in children.92
Missed appendicitis ranks in the top five causes of litigation against emergency physicians and accounts for 5% of all money paid out by insurers on their behalf.87 Although acute appendicitis is the most common surgical cause of abdominal pain in children, 88 it can be one of the most difficult diagnoses to make. The negative appendectomy rate in children is reported to be 20%-50%,58,89 and the incidence of perforated appendicitis in young children is 40%- 70%.10 In one small study, the perforation rate in children one year of age and under was 100%.11
While some cases of acute appendicitis present in the classic fashion, others demonstrate nonspecific historical, physical, and lab findings. The signs and symptoms of appendicitis overlap with the many benign causes of abdominal pain, especially gastroenteritis. About 30% of children with appendicitis have diarrhea, and the incidence of diarrhea increases in those with perforation.14
When the diagnosis is not made until after perforation has occurred, mortality and morbidity increase. Cases of appendicitis that result in litigation often involve abscess drainage and postoperative complications. 88 Not surprisingly, perforated appendicitis results in more litigation than nonperforated acute appendicitis. Claims of loss may even include future infertility in females from ruptured appendicitis.90
Other causes of abdominal pain share common themes with appendicitis with regard to medicolegal risk. That is, they are difficult to diagnose, occur commonly, and a delay in the diagnosis may increase the risk of a bad outcome. Intussusception is very difficult to diagnose, especially absent the triad of colicky, intermittent abdominal pain, vomiting, and bloody stools. A rectal examination revealing blood may be the only clue that a lethargic infant has intussusception and not sepsis. Early barium enema may reveal the diagnosis before significant bowel necrosis occurs.
The shy child with abdominal pain and vomiting may have testicular torsion that is only detected if the physician is careful to examine the genitals. Delay will result in loss of a testicle. Abuse must be considered, as this may prevent death or injury from future assaults. Diabetic ketoacidosis may present like gastroenteritis (or a surgical abdomen); an elevated blood glucose or abnormal urine dipstick may provide the diagnosis.
If the diagnosis remains in doubt, but the patient does not require additional testing or consultation, arrange for repeat evaluation in 8-12 hours. If the pain is relentless and the diagnosis is unclear, continued observation with repeat evaluations in the ED may be very helpful. In such cases, abdominal ultrasound or CT can help identify serious causes of abdominal pain, including those with unusual or rare diagnoses.1,91 If the child appears ill or has a worrisome examination, involve the surgical consultant at an early stage.
With these issues in mind, we offer the following strategies.
1. Rely on observation and repeat history and physical examination to make the diagnosis.
2. Pelvic and rectal examinations are cheap.
These exams can offer a wealth of information at minimal financial cost, especially if pelvic pathology or intussusception are clinically likely.
3. Minimize laboratory tests.
4. Urinalysis and urine pregnancy tests are relatively inexpensive.
5. Minimize abdominal films.
6. When the diagnosis is clearly surgical, consult the surgeon prior to ordering radiologic tests.
1. "The patient had diarrhea, so I just thought that it was gastroenteritis."
2. "I didn't think that a repeat exam was warranted. He looked so good the first time."
3. "There was no complaint related to the diaper area, so I didn't examine there."
4. "They seemed like such a nice family that I didn't even consider abuse."
5. "I just left it up to the family to take the patient to the pediatrician as needed."
6. "She said she had never had sex, so I didn't order a pregnancy test."
7. "He was so lethargic that I thought for sure he was septic."
8. "The child didn't say that it hurt when she urinated, so I didn't check the urine."
9. "It couldn't have been appendicitis. The white count was normal."
10. "He never said that he had had mononucleosis."
1. Is this teenage girl sexually active?
Concern: Ectopic pregnancy and pelvic inflammatory disease.
2. Does the pain come and go, or are the stools bloody, or has there been any change in mental status, in the young child?
Concern: Intussusception in the young child.
3. Is there localized pain and tenderness, especially on the right side?
Concern: Appendicitis.
4. Does the neonate have bilious vomiting?
Concern: Malrotation with midgut volvulus.
5. Is there a scrotal mass or discoloration?
Concern: Inguinal hernia, testicular torsion.
6. Is the child drinking or urinating more than usual?
Concern: Diabetic ketoacidosis.
7. Could this be a case of child abuse?
Concern: Concealed trauma.
8. Has there been a recent history of mononucleosis?
Concern: Rupture of the spleen—either spontaneous or traumatic.
9. Is there a history of immunosuppression or chronic steroid use?
Concern: Surgical disease despite a paucity of clinical findings.





Evidence-based medicine requires a critical appraisal of the literature based upon study methodology and number of subjects. Not all references are equally robust. The findings of a large, prospective, randomized, and blinded trial should carry more weight than a case report.
To help the reader judge the strength of each reference, pertinent information about the study, such as the type of study and the number of patients in the study, will be included in bold type following the reference, where available. In addition, the most informative references cited in the paper, as determined by the authors, will be noted by an asterisk (*) next to the number of the reference.
Lance Brown; Jonathan Jones
December 1, 2000
Accredited By





Our Partners


 678-366-7933
678-366-7933