Table of Contents
About This Issue
Acute bronchitis is a common presentation in urgent care and remains a clinical diagnosis characterized by acute cough that may last >3 weeks, often with sputum production and spontaneous resolution. Because symptoms overlap with more serious conditions, clinicians must carefully evaluate for “don’t-miss” diagnoses such as pneumonia, pulmonary embolism, and heart failure. Most cases are viral (>90%), making supportive care the cornerstone of treatment and reinforcing the importance of antibiotic stewardship. Evidence-based evaluation—focused on history, physical examination, and selective use of diagnostics—can reduce unnecessary testing and treatment while ensuring patient safety. Effective management also relies on clear patient education, symptom-based care, and appropriate return precautions, particularly in higher-risk populations such as the elderly or immunocompromised. In this issue, you will learn:
How to evaluate patients presenting in urgent care with cough and identify features consistent with acute bronchitis;
How to differentiate bronchitis from serious conditions such as pneumonia, pulmonary embolism, and heart failure;
Evidence-based approaches to utilizing diagnostic testing and recommending symptomatic management; and
Best practices for patient education, discharge instructions, and return precautions.
- About This Issue
- Abstract
- Case Presentations
- Introduction
- Etiology and Pathophysiology
- Differential Diagnosis
- Urgent Care Evaluation
- History
- Vital Signs
- Physical Examination
- Diagnostic Studies
- Laboratory Studies
- Imaging
- Treatment
- Symptomatic Treatment
- Contraindicated Treatments
- Antibiotics
- Antihistamines
- Expectorants
- Bronchodilators
- Corticosteroids
- Other Treatments
- Special Populations
- Immunocompromised Patients
- Older Patients
- Pregnant Patients
- Controversies and Cutting Edge
- Disposition
- Summary
- Critical Appraisal of the Literature
- Time- and Cost-Effective Strategies
- 5 Things That Will Change Your Practice
- Risk Management Pitfalls in the Management of Acute Bronchitis in Urgent Care
- KidBits: Urgent Care Management of Acute Bronchitis in the Pediatric Population
- Urgent Care Evaluation
- Pediatric Management
- Counseling Families About Bronchitis
- Key Points
- References
- Case Conclusions
- Coding & Charting: What You Need to Know
- Coding Challenge: Acute Bronchitis
- Clinical Pathway for Urgent Care Management of Acute Bronchitis
- References
Abstract
Acute bronchitis is common in the urgent care setting and is a clinical diagnosis. Patients typically present with acute onset of cough that has lasted for 1 to 3 weeks, and although symptoms resolve without intervention, it is important to consider and evaluate for “don’t-miss” diagnoses and disease processes that can mimic acute bronchitis. Treatment is largely supportive, and antibiotics should not be given for most patients with acute bronchitis. Patients should also receive education about their illness and should be provided with strict return precautions. By following evidence-based recommendations for the diagnosis and management of acute bronchitis, urgent care clinicians can avoid ordering unnecessary tests and medications.
Case Presentations
- His cough is productive of clear yellow sputum. He has not experienced any chest pain, shortness of breath, fever, edema, or posttussive emesis.
- His past medical history is significant for type 2 diabetes mellitus, obesity, and hypercholesterolemia, and he is taking metformin and rosuvastatin.
- On examination, his lungs are clear to auscultation bilaterally, and the rest of his examination is unremarkable.
- His vital signs are: temperature, 36.9°C; heart rate, 88 beats/min; blood pressure, 134/85 mm Hg; respiratory rate, 16 breaths/min; and O2 saturation, 98% on room air.
- You consider what could be causing his cough…
- Her physical examination is notable for bilateral scattered wheezes on lung auscultation. When asked to cough, her wheezing partially resolves.
- She has a past medical history of hypertension, hyperlipidemia, and generalized anxiety disorder. She is taking lisinopril, atorvastatin, and sertraline.
- Her vital signs are: temperature 37.2°C; heart rate, 92 beats/min; blood pressure, 141/88 mm Hg; respiratory rate, 14 breaths/min; and O2 saturation, 99% on room air.
- You consider whether this patient has an infection that requires antibiotics and question what your workup should include…
- She is now requiring 4L of oxygen to maintain saturation between 88% and 92%.
- She has a cough productive of sputum and has had fevers, with a maximum temperature at home of 100.9°F.
- She has a past medical history of COPD (on 2L of oxygen at home), hypothyroidism, hypertension, and hyperlipidemia. She is taking a combined daily fluticasone/umeclidinium/vilanterol inhaler, levothyroxine, amlodipine, and atorvastatin.
- Her physical examination is notable for bilateral wheezing on lung examination.
- Her vital signs are: temperature, 38.4°C; heart rate, 108 beats/min; blood pressure, 110/76 mm Hg; respiratory rate, 24 breaths/min; and O2 saturation, 90% on 4L nasal cannula.
- You consider what your next steps for this patient should be…
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
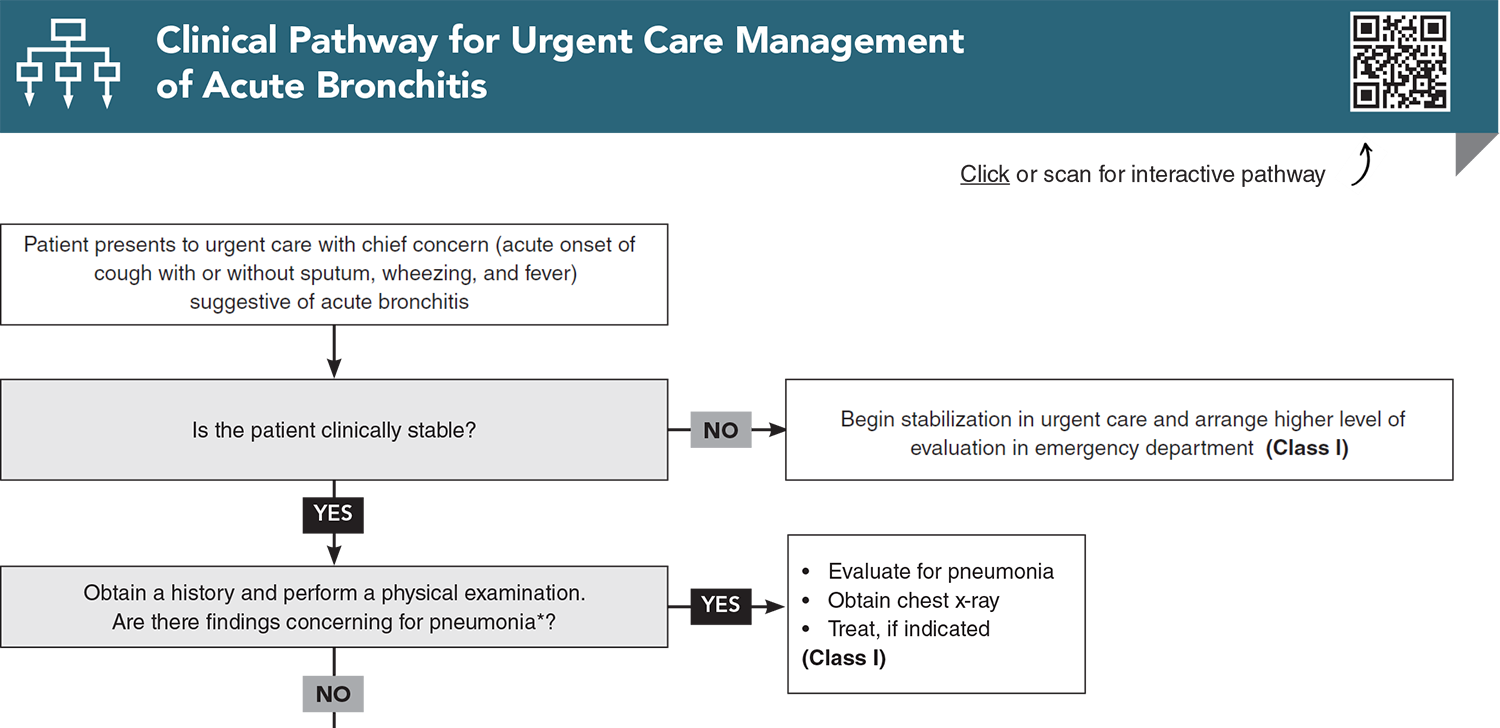
Clinical Pathway for Urgent Care Management of Acute Bronchitis
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Buy this issue and
CME test to get 4 CME credits.
Key References
Following are the most informative references cited in this paper, as determined by the authors.
1. * Mulhem E, Patalinghug E, Eraqi H. Acute bronchitis: rapid evidence review. Am Fam Physician. 2025;111(3):214-217. (Review)
2. * Miller JM, Binnicker MJ, Campbell S, et al. Guide to utilization of the microbiology laboratory for diagnosis of infectious diseases: 2024 update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). Clin Infect Dis. 2024:ciae104. (Expert consensus guideline) DOI: 10.1093/cid/ciae104
3. * Harris AM, Hicks LA, Qaseem A, et al. Appropriate antibiotic use for acute respiratory tract infection in adults: advice for high-value care from the American College of Physicians and the Centers for Disease Control and Prevention. Ann Intern Med. 2016;164(6):425-434. (Clinical practice guideline) DOI: 10.7326/m15-1840
6. * Park JY, Park S, Lee SH, et al. Microorganisms causing community-acquired acute bronchitis: the role of bacterial infection. PLoS One. 2016;11(10):e0165553. (Prospective observational study; 811 patients) DOI: 10.1371/journal.pone.0165553
7. * Gonzales R, Sande MA. Uncomplicated acute bronchitis. Ann Intern Med. 2000;133(12):981-991. (Review) DOI: 10.7326/0003-4819-133-12-200012190-00014
19. * Smith MP, Lown M, Singh S, et al. Acute cough due to acute bronchitis in immunocompetent adult outpatients: CHEST expert panel report. Chest. 2020;157(5):1256-1265. (Practice guideline) DOI: 10.1016/j.chest.2020.01.044
23. * Ebell MH, Merenstein DJ, Barrett B. Corticosteroids, antitussives, and inhalers for lower respiratory tract infections in US primary care: a prospective cohort study. J Gen Intern Med. 2025. (Prospective cohort study; 718 patients) DOI: 10.1007/s11606-025-09733-x
Subscribe to get the full list of 32 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: acute bronchitis, cough, upper respiratory tract infection, inflammation, mucus, bronchi, sputum, wheezing, rhonchi, supportive care, home remedies, virus, pertussis, vaccination, honey, hydration, cough drops, saline nasal spray, antibiotic stewardship









 678-366-7933
678-366-7933