Table of Contents
About This Issue
Acute asthma exacerbations are common and potentially high-risk urgent care presentations requiring rapid clinical assessment, prompt evaluation and treatment, and thoughtful disposition. Asthma exacerbations are primarily diagnosed clinically, with attention to severity markers such as oxygen saturation, respiratory rate, accessory muscle use, ability to speak, wheezing or “silent chest,” and response to initial therapy. Because dyspnea and wheezing overlap with serious alternative diagnoses, clinicians must consider other high-risk conditions. In-office management centers on prompt use of oxygen when indicated, short-acting beta agonists, anticholinergics for moderate to severe exacerbations, and early systemic corticosteroids. Discharge planning is equally important, as current guidelines discourage SABA-only treatment to reduce relapse. In this issue, you will learn:
To classify acute asthma exacerbations as mild, moderate, or severe;
How to distinguish asthma exacerbation from serious mimics such as COPD, heart failure, pneumonia, pulmonary embolism, and pneumothorax;
Evidence-based approaches to urgent care treatment; and
Best practices for discharge planning, including assessment for prescribing an at-home regimen, patient education regarding inhaler technique, follow-up, and return precautions.
CODING & CHARTING: Check out the monthly coding column, which includes important details about documenting and coding for acute asthma exacerbations.
- About This Issue
- Abstract
- Case Presentations
- Introduction
- Epidemiology
- Prevalence of Asthma and Healthcare Costs
- Social Determinants and Risk Factors
- Etiology and Pathophysiology
- Differential Diagnosis
- Congestive Heart Failure
- Chronic Obstructive Pulmonary Disease
- Pulmonary Embolism
- Other Conditions in the Differential for Asthma
- Urgent Care Evaluation
- History
- Physical Examination
- Classifications of Asthma Exacerbation
- Mild Exacerbation
- Moderate Exacerbation
- Severe Exacerbation
- Diagnostic Studies
- Laboratory Evaluation
- Point-of-Care Ultrasound
- Peak Expiratory Flow
- Chest Radiographs
- Treatment
- Management of the Acute Exacerbation Presenting to Urgent Care
- Oxygen
- Pharmacologic Agents
- Beta Agonists
- Metered-Dose Inhalers Versus Nebulizers
- Intermittent Versus Continuous Nebulizer Treatments
- Anticholinergics
- Corticosteroids
- Magnesium Sulfate
- Epinephrine
- Postdischarge Care/Aftercare
- At-Home Reliever Inhaler Strategy for Asthma Management
- Reducing Exacerbations to Minimize Oral Corticosteroid Exposure
- Special Populations
- Pregnant Patients
- Asthma Patients With COVID-19
- Athletes With Exercise-Induced Bronchospasm
- Controversies and Cutting-Edge
- Biologics
- Red-Tape Challenges for Inhaled Corticosteroids
- Disposition
- Indications for Referral for Emergency Department Evaluation
- Time- and Cost-Effective Strategies
- Summary
- Risk Management Pitfalls for Management of Acute Asthma Exacerbations in Urgent Care
- KidBits: Asthma in Pediatric Patients
- Urgent Care Diagnosis
- Treatment
- Discharge Planning
- References
- Case Conclusions
- Coding & Charting: What You Need to Know
- Number and Complexity of Problems Addressed
- Amount and/or Complexity of Data to be Reviewed and Analyzed
- Risk of Complications and/or Morbidity or Mortality of Patient Management
- Documentation Tips
- Coding Challenge: Acute Asthma Exacerbations in Urgent Care
- Clinical Pathways
- Clinical Pathway for Management of Asthma Exacerbations in Adult Patients in the Urgent Care Setting
- Clinical Pathway for Management of Asthma Exacerbations in Pediatric Patients in the Urgent Care Setting
- References
Abstract
Asthma is a disease of the airways characterized by inflammation, hyperresponsiveness, and bronchoconstriction. The diagnosis of acute asthma exacerbation is primarily a clinical one, based on a focused history and physical examination. It is important to differentiate it from other entities such as heart failure, pneumonia, and pulmonary embolism, which can present with similar respiratory signs. Urgent care asthma management is focused on rapid stabilization of acute exacerbation, followed by reinforcement and optimization of the patient's asthma management plan to prevent relapse risk and repeat visits. Inhaled corticosteroids are now recommended as part of the at-home treatment for asthma across all severities. This issue reviews the latest evidence in diagnostic and treatment strategies, including other pharmacologic treatments and newer management strategies.
Case Presentations
- He has a history of frequent urgent care visits for asthma, including multiple hospital admissions and intubations.
- The patient is slightly tachypneic and not using accessory muscles to breathe. On auscultation, air entry is significantly diminished bilaterally, and he has faint expiratory wheezing bilaterally.
- His vital signs are: blood pressure, 155/85 mm Hg; heart rate, 120 beats/min; respiratory rate, 20 breaths/min; temperature, 36.9°C; and oxygen saturation, 91% on room air.
- You recognize that this patient needs ED management but consider what interventions are needed while you await transport…
- The patient says she discontinued her asthma medications because she has not used them in the past 2 years.
- Her vital signs are: blood pressure, 120/75 mm Hg; heart rate, 80 beats/min; respiratory rate, 18 breaths/min; and room-air pulse oximeter reading, 97%.
- On auscultation she has faint diffuse wheezing with good air movement.
- You consider the treatment options for this patient…
- Upon discharge, he asks, "Can you refill my albuterol inhaler?"
- He does not have any respiratory symptoms currently.
- You mentally question if he is on the correct treatment and whether you should refill his inhaler...
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
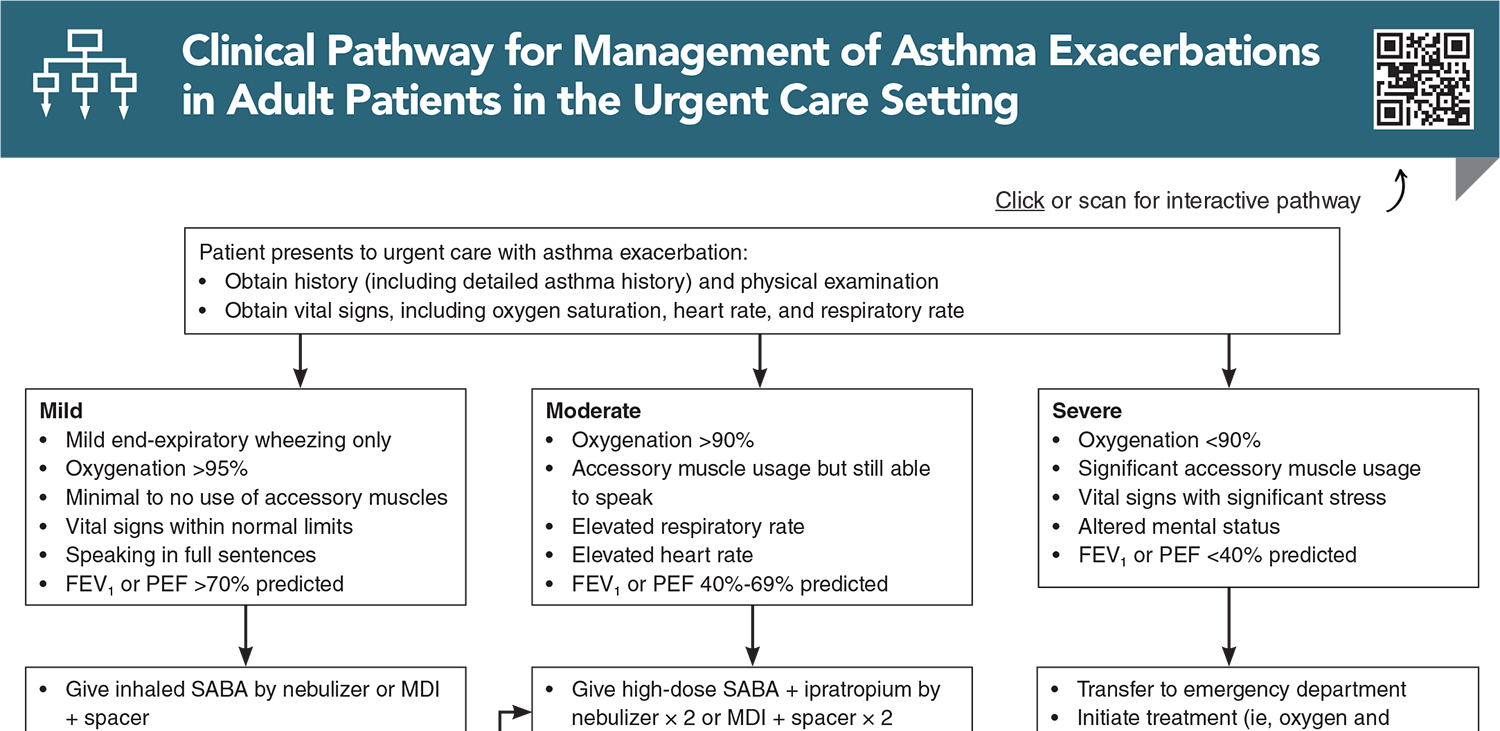
Clinical Pathway for Management of Asthma Exacerbations in Adult Patients in the Urgent Care Setting
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
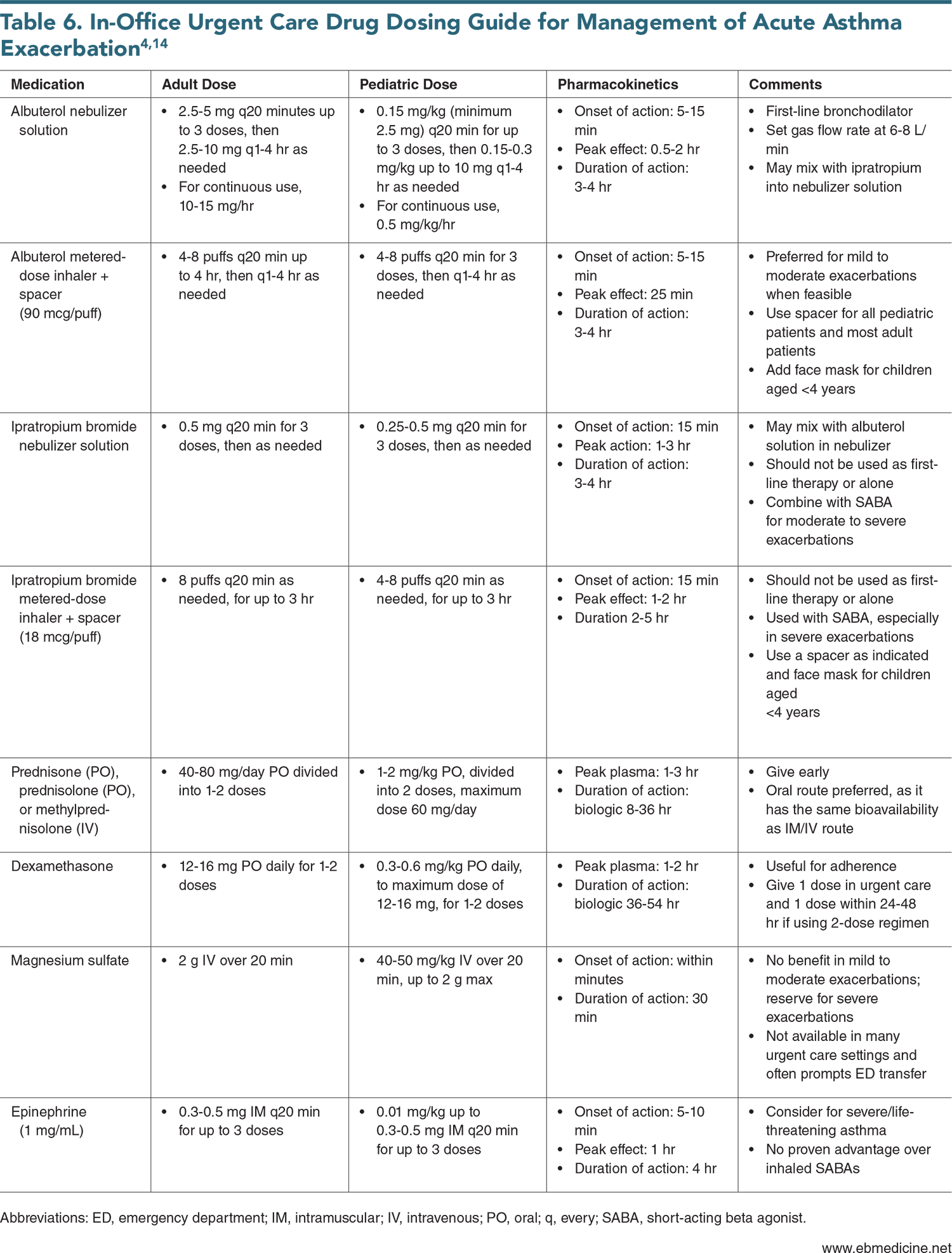
Tables and Figures
Subscribe for full access to all Tables and Figures.
Buy this issue and
CME test to get 4 CME credits.
Key References
Following are the most informative references cited in this paper, as determined by the authors.
4. * Global Initiative for Asthma. Global strategy for asthma management and prevention (2026 update). Accessed May 15, 2026. (Clinical practice guidelines)
11. * National Asthma Education and Prevention Program, Third Expert Panel on the Diagnosis and Management of Asthma. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: United States Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute; 2007. (Clinical guidelines)
15. * Padem N, Saltoun C. Classification of asthma. Allergy Asthma Proc. 2019;40(6):385-388. (Review) DOI: 10.2500/aap.2019.40.4253
29. * Scottish Intercollegiate Guidelines Network, British Thoracic Society. British guideline on the management of asthma: a national clinical guideline. 2003. Revised July 2019. Accessed May 15, 2026. (Clinical guidelines)
Subscribe to get the full list of 96 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: acute asthma exacerbation, asthma management, dyspnea, wheezing, bronchoconstriction, airway inflammation, hyperresponsiveness, shortness of breath, cough, chest tightness, short-acting beta agonist (SABA), inhaled corticosteroids (ICS), metered-dose inhaler (MDI), MDI with spacer, nebulizer, anticholinergics, systemic corticosteroids, oxygen therapy, peak expiratory flow (PEF), pulse oximetry, exacerbation, silent chest, respiratory distress, relapse prevention









 678-366-7933
678-366-7933