Ultrasound In The Evaluation Of Thoracic Trauma
Ultrasound has been shown to be more sensitive than supine AP chest radiograph for the detection of traumatic pneumothoraces69and ultrasound is useful for the detection of hemothorax. In some centers, thoracic ultrasound is performed routinely along with the traditional FAST scan, creating the extended focused abdominal sonogram for trauma (EFAST).70
Ultrasonography has been reported to have greater sensitivity in detecting chest wall fractures than either clinical acumen or radiography; 80% vs 26% vs 24%.76In addition to rib fractures, this includes sternal fractures. While not commonly used for this purpose in the United States, ultrasound is a rapid and reliable method for identifying bony disruptions, especially in the superficial, readily accessible ribs and sternum.77 This application represents an opportunity for additional study by emergency ultrasound researchers.
In the past, the literature has stressed the importanceof rib fractures, especially those of the first andsecond ribs, as predictors of aortic injury. However, several studies have demonstrated no increased likelihood of aortic injury with upper rib fractures.2,75No additional imaging studies are mandated by thesefindings alone.
Significance And Diagnosis Of Myocardial Contusion
The clinical significance of myocardial contusion following blunt chest trauma is unknown. A number of diagnostic approaches have been used for diagnosis, including electrocardiography, serial enzyme measurement, and both TTE and TEE. TTE has proven inadequate, but TEE appears to be safe and to provide excellent quality images. Based on a retrospective study of 81 patients who received TEE in the evaluation of blunt chest trauma, Weiss et al found myocardial contusions, diagnosed by wall motion abnormalities, in almost a quarter of these patients. They noted an increase in mortality rate associated with this diagnosis.95However, a more recent prospective study by Lindstaedt et al of 180 patients with blunt chest trauma found only a 12% incidence of myocardial contusion, and none of their patients experienced any cardiac complications. They concluded that myocardial contusion is a frequent finding in polytraumatized patients, but that the outcome and prognosis is favorable.96
Since first generation scanners missed approximately a third of pulmonary emboli in one study, they could not be used alone to diagnose or exclude pulmonary embolism.27Additional tests that have been used in conjunction with early generation CT scanners included serial venous ultrasonography of the legs30 and CT venography of the pelvis and legs.31,109 With advanced generation scanners, it now appears feasible to use clinical risk stratification, D-dimer measurement, and multi-detector CT scanning to reliably and safely diagnose or exclude clinically significant pulmonary emboli.34-37A systematic review published in 2005 of 15 studies published between 1990 and 2004 containing 3500 patients found that the use of CT ruled out pulmonary embolism. An overall negative predictive value of 99.1% for a chest CT negative for pulmonary embolism was found, even though all generations of scanners were included in the review. This is a similar negative predictive value as that for conventional pulmonary arteriography. Furthermore, the use of advanced generation scanners should improve the negative predictive value.32
The chest radiograph is often included in the work-up of the hypertensive patient, presumably to evaluate for the presence of LVH. However, the CXR is insensitive for the detection of LVH and is not clearly indicated in uncomplicated cases.7 CXR is possibly indicated in patients with moderate to severe hypertension and probably should be reserved for patients with cardiorespiratory symptoms or signs.7,146 Echocardiography is the non-invasive modality of choice for the detection of the cardiac effects of systemic hypertension, the most common cause of LVH. 147,40
The Role Of CT In The Evaluation Of Pulmonary Infection In Immunocompromised Patients
If there is a high clinical suspicion for a pulmonary infection in the setting of a normal chest radiograph, a high-resolution, non-contrast CT scan may be warranted to assess for subtle abnormalities. Patients who have a normal chest radiograph and PCP will usually exhibit focal areas of ground-glass opacity on CT.5x
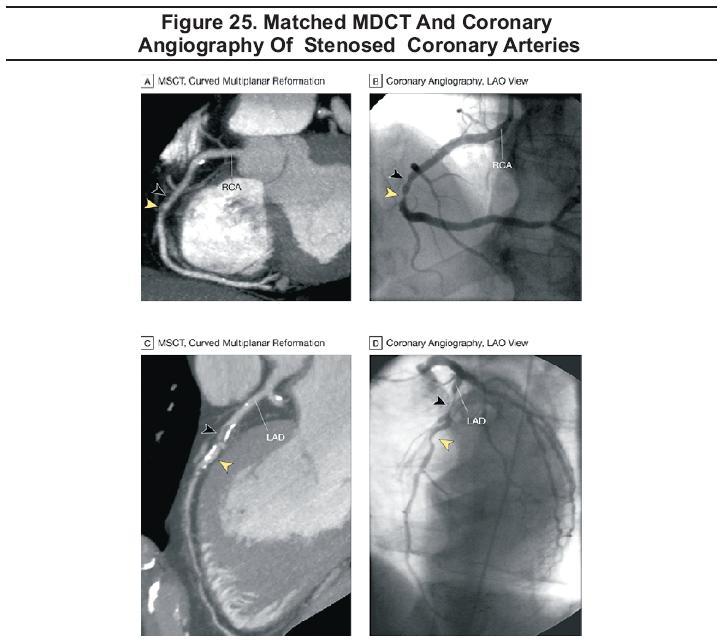
The Role Of CT In The Diagnosis Of Coronary Artery Stenosis
Electron beam computed tomography (EBCT) has been in use for many years as a means of measuring coronary artery calcium and estimating the overall coronary atherosclerotic plaque burden. EBCT has proven useful in identifying individuals with or at risk for coronary heart disease. However, there is still controversy as to the prognostic significance of calcium, as some investigators believe that the presence of coronary calcification may stabilize the atherosclerotic plaque.135
High-resolution images obtained rapidly by MDCT have recently improved image quality to the point where it may soon be possible to consider non-invasive coronary angiography as a routine clinical tool.48MDCT shows promise as a means of excluding coronary artery stenosis in a non-invasive fashion (Figure 25). Reports of the use of 16-slice MDCT for non-invasive coronary angiography have been appearing in the literature since 2002, and in 2005, reports of the use of 64-slice MDCT began to appear.
Gary R Strange; Bruce MacKenzie
November 1, 2006
Wrist Injuries Emergency Imaging And Management
Emergency Imaging For The 21st Century: Where Does Ultrasound Fit In?
An Evidence-Based Approach To Imaging Of Acute Neurological Conditions
Imaging In The Adult Patient With Nontraumatic Abdominal Pain
Accredited By





Our Partners

