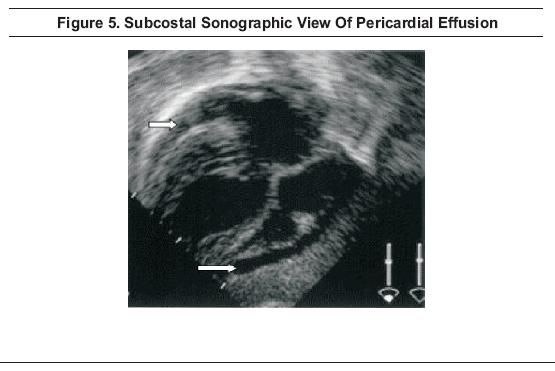
The portable AP chest radiograph, along with a lateral cervical spine film and AP pelvis, remains a part of the screening radiology evaluation for the blunt multisystem trauma patient, as recommended by the American College of Surgeons Advanced Trauma Life Support Course.1In addition, the focused abdominal sonogram for trauma (FAST) is recommended not only for the evaluation of potential intra-abdominal injury but for the evaluation of the pericardial sac (Figure 5).1,66-68
In addition to the sub-costal view of the heart and pericardium, standard views include the right upper quadrant, the left upper quadrant, and the pelvis. Views of the right and left paracolic gutters are often added and it may be possible to visualize blood superior to the hyperechoic diaphragm in the presence of hemothoraces. While the FAST exam is relatively reliable in detecting free intraperitoneal blood, it has limited utility in detecting solid organ injury or retroperitoneal bleeding.
Ultrasound has been shown to be more sensitive than supine AP chest radiograph for the detection of traumatic pneumothoraces69 and, in some centers, thoracic ultrasound is performed routinely along with the traditional FAST scan, creating the extended focused abdominal sonogram for trauma (EFAST).70
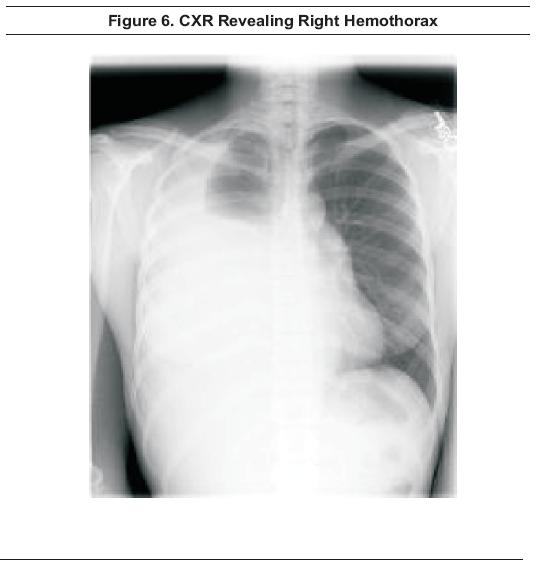
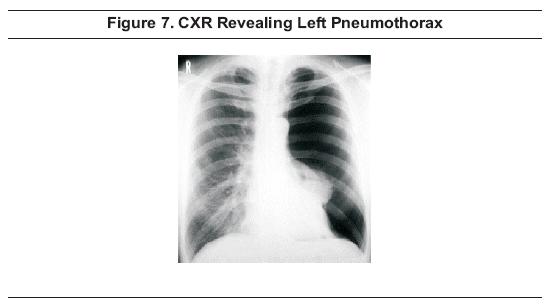
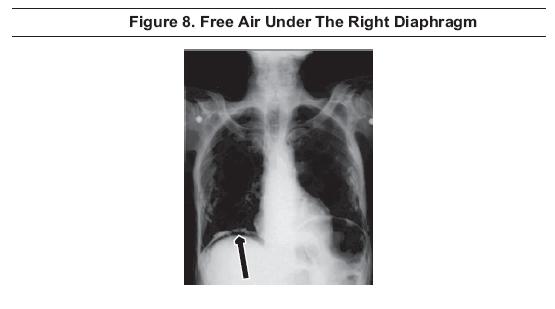
In the setting of penetrating trauma, no imaging is required if the patient is hemodynamically unstableand does not respond to resuscitation with crystalloids and blood. Operative intervention is required in these cases. In stable patients with penetration above the umbilicus or for those with suspected thoracoabdominal injury, an upright CXR is the most commonly used study to evaluate for the presence of hemothorax (Figure 6), pneumothorax, (Figure 7), or intraperitoneal air (Figure 8). Serial CXR's may be used when suspicion is high and initial screening radiographs are negative.1 Using the supine AP CXR, the presence of subcutaneous emphysema or the radiographic deep sulcus sign may be useful in diagnosing small pneumothoraces. The deep sulcus sign is detected by noting lucency and a sharp, angular appearance of the costophrenic angle on the involved side.71
However, some studies showed that ultrasound is more sensitive than the CXR in diagnosing pneumothoraces69 and hemothoraces.8 An ultrasonic deep sulcus sign may be noted sonographically.72
As with blunt trauma, the FAST scan is used to evaluate the pericardial sac (Figure 5) and to assess for blood in Morison's pouch (the hepatorenal interface), the splenorenal interface, and in the pelvic spaces; the EFAST scan can be used to evaluate the thorax simultaneously. 1,70
MDCT scan is superior to supine chest radiographs in diagnosing pulmonary contusion. On CT, contusions appear as patchy or diffuse air space filling that tends to be peripheral, nonsegmental, and geographic in distribution. CT is also the imaging study of choice for transmediastinal gunshot wounds, since CT is able to visualize wounds that penetrate the great vessels, pericardium, esophagus, trachea, and thoracic spine. CT is less expensive, less time-consuming, and less invasive than angiography or endoscopy and these tests can generally be avoided if MDCT confirms that the wound track does not come in close proximity to these structures.73
Rib views have traditionally been used for detection of rib fractures in patients who have been subjected to direct blows or compressive injuries to the chest, but often add little to the management of the patient. The ACR rates specialized rib views as having a low level of appropriateness (2/9) for adults less than 65 years of age.2While not specifically indicated, the ACR rates these views at a moderate level of appropriateness (5/9) for adults greater than 65 years of age.
The ACR recommends rib views as more appropriate for children under 14 years of age (8/9) since children have more compliant rib cages and the presence of fracture(s) is associated with significant trauma and increased associated injury. In children less than three years of age, rib fractures are frequently a marker of abuse.74
The chest radiograph is appropriate at any age (8 to 9/9) when the diagnosis of rib fracture is under consideration, and is primarily used to rule out associated pulmonary injury.2
In the past, the literature has stressed the importance of rib fractures, especially those of the first and second ribs, as predictors of aortic injury. However, several studies have demonstrated no increased likelihood of aortic injury with upper rib fractures.2,75 No additional imaging studies are mandated by these findings alone.
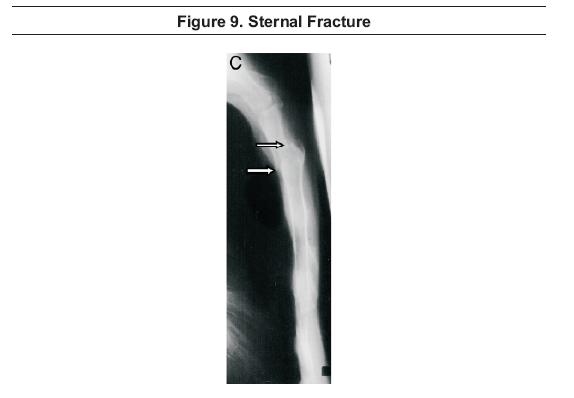
Sternal fractures (Figure 9) are reported to be associated with severe injuries. In a retrospective review of 200 sternal fractures, von Garrel et al reported injuries to the thoracic vasculature, including the heart, in approximately 30% of cases, and such injuries were increased with displacement of sternal fragments. Fatal heart injuries were frequently seen in conjunction with sternal fractures in patients who fell from significant heights. Spinal injuries were associated with sternal fractures in 13% of cases and were most likely in fractures with involvement of the manubriosternal joint.78
Hemothorax is most often detected by the finding of fluid in the pleural cavity on screening CXR (Figure 6). However, ultrasonography can detect hemothoraces not evident on CXR and is rapid and accurate; sensitivity of ultrasound is reported at 92%, specificity at 100%, positive predictive value at 100%, and negative predictive value at 98%.79, 80
Angiography plays a role in the evaluation of the patient with hemothorax and may identify occlusion, active hemorrhage, or pseudoaneurysm. A potential advantage of angiography is that, when specific bleeding sites are identified, one can proceed to selective embolization of the internal mammary or intercostal artery, which may be an effective alternative to thoracotomy.81,82 While this treatment modality is promising, the number of cases studied is small.
Further study is needed before firm recommendations can be made.
The primary modality currently used for detection of pneumothorax or pneumomediastinum is the CXR (Figure 7). Inspiratory and expiratory views probably do not improve the detection of pneumothoraces above the standard CXR.83,84,85 A prospective, randomized review of 178 patients paired inspiratory and expiratory chest radiographs with and without pneumothoraces; inspiratory and expiratory upright films were found to be equally sensitive for pneumothorax detection.84 Films must be perused carefully since small pneumothoraces can easily be missed and overlying skin folds can simulate pneumothoraces. Ultrasound is more sensitive than AP CXR for the detection of pneumothorax and demonstrates good agreement with CT scan.69
Pneumopericardium
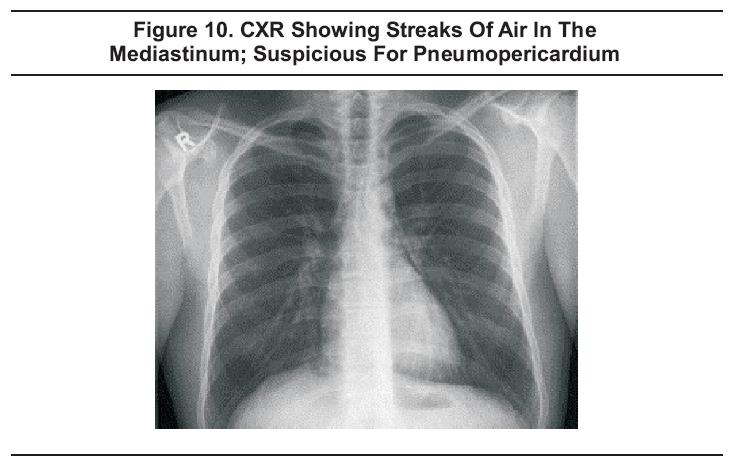
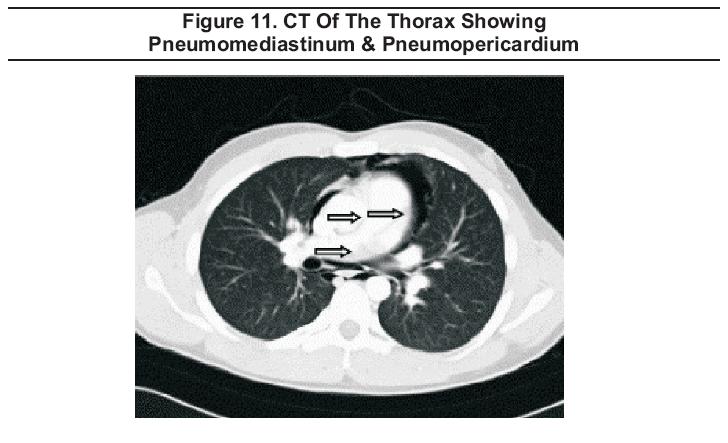
Pneumopericardiummay result from blunt chest trauma, pneumothorax, pneumoperitoneum, pneumomediastinum, tracheobronchial tears, or esophageal tears. It may be seen on CXR (Figure 10), but is best diagnosed using CT scan of the thorax and abdomen (Figure 11) which allows for the additional detection of concomitant injuries.86,87
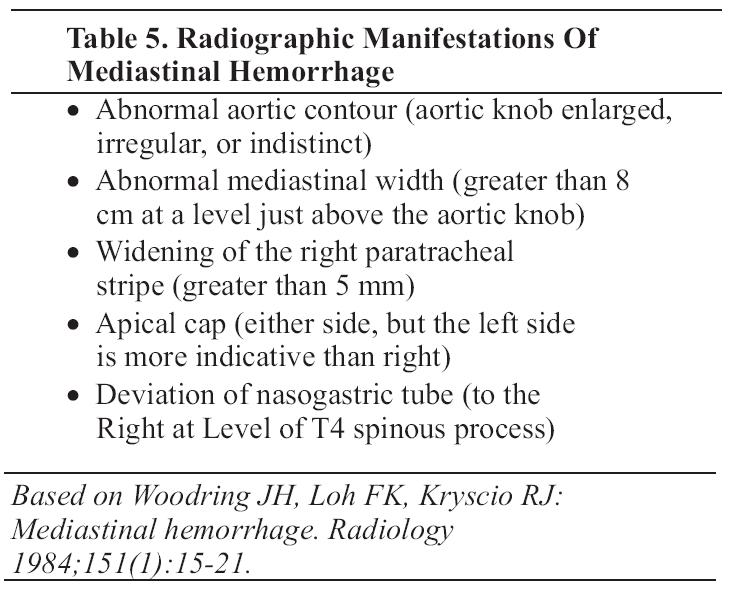
Hemorrhage into the mediastinum is suspected when the supine AP CXR shows abnormal mediastinal contours (Figure 12). A number of radiographic findings have been promulgated as indicative of mediastinal hemorrhage, but, in a study comparing radiograph interpretation in normal patients and patients with mediastinal hemorrhage, Woodring found only five signs to be helpful; see Table 5.88 The aortic contour is considered to be abnormal when the aortic knob is enlarged, irregular, or indistinct. The mediastinum is considered to be widened on the supine AP CXR when the width is 8 cm or greater when measured just above the aortic knob. An apical cap is formed when blood dissects above the lung on either side; but a left apical cap is more indicative of mediastinal bleeding than one on the right. Displacement of a nasogastric tube to the right at the level of T4 is also suggestive of a mediastinal hematoma. The right paratracheal stripe is a space between the right tracheal wall and the adjacent lung and pleura. With hemorrhage into the mediastinum, this potential space can fill with blood and become distended. Based on a study of 102 consecutive patients using thoracic arteriograms as the gold standard, widening to greater than 5 mm is suggestive of mediastinal hemorrhage; a paratracheal stripe was reported to be associated with major arterial injury in 23% of cases.89

CT of the chest is 100% sensitive and 99.7% specific for mediastinal hemorrhage. The positive predictive value is 89% while the negative predictive value is 100%, giving an overall diagnostic accuracy of 99.7%.90 CT is accurate for the detection and localization of both hemomediastinum and direct signs of aortic injury, and has largely supplanted aortography for the diagnosis of these problems.90
Chest radiography is frequently used as an initial screening tool in patients with possible aortic injury, but there are no CXR findings with both high sensitivity and high specificity for aortic injury. A mediastinum greater than 8 cm at the level of aortic knob (Figure 12) has a sensitivity greater than 90% but a low specificity. Thoracic spine fracture, first rib fracture, rightward deviation of a nasogastric tube, depression of the left mainstem bronchus, and widened paraspinal line are all findings with specificity greater than 90% but low sensitivity, and no significant improvement in overall accuracy was achieved by combining radiographic findings.91False positive and false negative findings occur with each x-ray sign, and in 1 to 2% of cases, the supine AP CXR is normal in the presence of a great vessel injury.92
As follow up for an abnormal CXR, computed tomography of the chest has a sensitivity of 100% and specificity of 99.7%.90
When there is evidence of aortic injury on CT, either aortography or surgery is indicated. An aortogram is useful when there is evidence of mediastinal hematoma adjacent to the aorta, but no aortogram is required for negative CT or for hematomas not adjacent to the aorta.90
A retrospective review of 200 patients with chest trauma found that pulmonary contusion (Figure 13) was the most common thoracic injury.93

CT gives the ability to better define the extent of the injury. Contusions appear radiodense and are usually peripheral, nonsegmental and nonlobar. The increased lung density is due to distal lung hemorrhage and edema.94
In the setting of penetrating trauma to the heart or lung, evaluation for pericardial hemorrhage is best carried out by echocardiography. The best view is the subcostal view in which fluid or blood will appear as an anechoic area surrounding the heart (Figure 5). Fluid will collect posteriorly first. If seen only anteriorly, the finding may be due to fatty deposition. Other potentially useful views are the parasternal long axis, parasternal short axis, and apical views. Sensitivity is reported to be 100% and specificity is 96.9% to 100%.97,98
Cardiac tamponade is a cardiovascular emergency requiring rapid diagnosis.99Sonographic criteria for the diagnosis of tamponade include diastolic collapse of the right ventricle or right atrium, possible collapse of the left atrium and ventricle, and distended inferior vena cava without respiratory variation. Transthoracic drainage under ECHO guidance is the recommended treatment, and has largely replaced the standard "blind" subxiphoid approach to pericardiocentesis commonly employed in the past.100
In the setting of tracheobronchial injury, lateral neck films may show air in soft tissues. CXR may show pneumomediastinum or pneumothorax ( Figure 7 ).101 CT of the chest with 3-D reconstruction of the tracheobronchial tree may be equivalent or superior to bronchoscopy.102,103
Esophageal Tears
Based on a retrospective review of 14 patients with esophageal perforation, Ghanem et al reported that the most common CXR finding was pleural effusion (64%), which was bilateral 60% of the time. When the effusion was unilateral, it was more commonly on the left. Pulmonary infiltrates were present in 64% of the cases and were most commonly bilateral. If unilateral, left-sided infiltrates were more common. Other CXR findings included pneumomediastinum (21%), pneumothorax (14%), and pneumopericardium (14%). Esophagography is indicated when an esophageal tear is suspected.86 The initial study should use water-soluble contrast medium, followed by a barium study if the water-soluble contrast study is negative. Positive findings on either study include extravasation (64%) and submucosal contrast medium collection (36%). Historically, endoscopy has been recommended if there is a high probability of injury and negative esophagography. However, CT has been shown to have sensitivity and specificity of 100% after suspected perforation.104CT findings of mediastinitis include increased attenuation of mediastinal fat (100%), pleural effusions (85%), free mediastinal gas bubbles (58%), localized mediastinal fluid collections (55%), sternal dehiscence (40%), mediastinal lymph nodes (35%), lung infiltrates (35%), pericardial effusion (28%), and pleuromediastinal fistula (3%).104
According to ATLS, CXR findings consistent with diaphragmatic injury include elevation or blurring of the diaphragm (Figure 14), hemothorax, abnormal gas shadow obscuring the hemidiaphragm, or gastric tube positioned in the chest.1

Findings on CT are similar. Based on the review of CT examinations of 179 patients with blunt trauma, Nchimi et al reported the following findings as strong predictors of blunt diaphragmatic rupture: Discontinuity, thickening, segmental non-recognition, intrathoracic hernia of abdominal viscera, elevation, hemothorax, and hemoperitoneum. Although not yet validated by other studies, the combination of discontinuity, thickening, and segmental nonrecognition was reported to be 100% sensitive.105 While CXR findings, especially displacement of a gastric tube, may be diagnostic of diaphragmatic injury, CT increases the accuracy of the diagnosis significantly.105
Gary R Strange; Bruce MacKenzie
November 1, 2006
Wrist Injuries Emergency Imaging And Management
Emergency Imaging For The 21st Century: Where Does Ultrasound Fit In?
An Evidence-Based Approach To Imaging Of Acute Neurological Conditions
Imaging In The Adult Patient With Nontraumatic Abdominal Pain
Accredited By





Our Partners

