ACR's Appropriateness Criteria rates CXR as highly appropriate (8/9) for most patients with a complaint of dyspnea regardless of physical findings, other symptoms, or risk factors for cardiopulmonary disease.3 CXR may demonstrate pulmonary infiltrates, vascular congestion, pneumothorax, pleural effusions, or neoplastic disease. Indirect evidence of thromboembolic disease may also be seen. For those under the age of 40 with a negative physical examination, the appropriateness is described as being influenced by severity and duration of dyspnea and the presence of other symptoms or risk factors for cardiovascular, pulmonary, and neoplastic diseases.3 While CT is not recommended for the initial evaluation of patients with dyspnea, except for patients with suspected pulmonary embolism, the ACR rates CT as appropriate (8/9) at any age when clinical evaluation, plain films, and laboratory studies are non-diagnostic.3 Plain CT is useful for detecting many diseases that may present with dyspnea, such as emphysema, sarcoidosis, and lung cancer.
Ventilation/perfusion (V/Q) lung scanning has been the primary tool for imaging pulmonary embolism in the past. In the Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED) study, the sensitivity of a normal or near-normal V/Q scan was shown to be 99%, with specificity of 98%. However, 78% of scans were read as low or intermediate probability. In addition, the overwhelming majority of patients without pulmonary embolism still had abnormal scans.23 V/Q scans require two hours to perform. One advantage is that V/Q scans result in less exposure to ionizing radiation than CT scans so they may be considered more useful for pregnant patients and patients that cannot tolerate intravenous contrast due to hypersensitivity or renal insufficiency.23
CT angiography of the chest has several advantages over either V/Q scanning or pulmonary angiography in the evaluation of the patient with possible pulmonary embolism. It is faster than either V/Q scanning or angiography. It is more practical in dyspneic patients and requires less contrast than angiography. It is generally more available than V/Q scanning or angiography and it may detect other important diagnoses when pulmonary embolism is not present24.
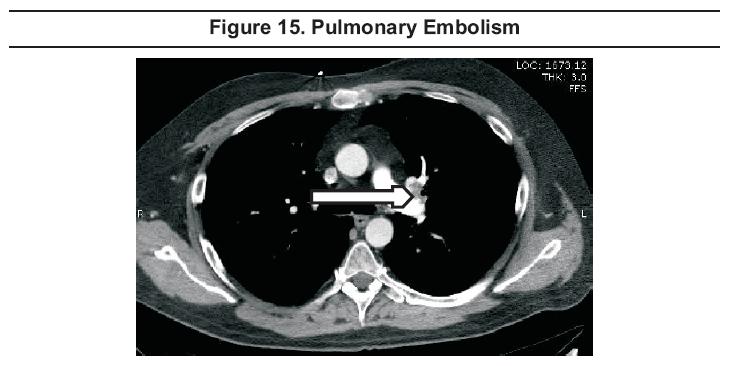
By 2001, CT scanning was being used more than lung scanning to investigate suspected pulmonary embolism.25Even with older generation scanners, CT could image from the main pulmonary arteries to the segmental and possibly sub-segmental arteries (Figure 15),24 but inter-observer agreement was poorer for sub-segmental arteries26.
With 16-slice multidetector-row CT scanners now commonly available, the entire chest can be imaged with excellent resolution, requiring a breath-hold of less than 10 seconds. These scanners can reliably diagnose tiny emboli in sub-segmental vessels.106 The clinical significance of sub-segmental emboli is unclear. In a study that included 67 patients with isolated subsegmental pulmonary emboli, Eyer et al reported that 37% did not receive anticoagulation and that there was no evidence of recurrent thromboembolism on follow up.107 Further study to confirm these findings is needed.
A positive CT result is an intraluminal filling defect or vascular occlusion24 (Figure 15).
Reported sensitivities vary widely, being affected significantly by the
generation of scanner used. While large series using specific
generations of scanners are yet to be published, Russo et al published
a meta-analysis of the relevant literature from 1995 to 2004. This
review showed the sensitivity and specificity to have increased from 37
to 94% and from 81 to 100% respectively, primarily due to the
possibility of depicting subsegmental clots.108
The PIOPED II trial was a prospective, multicenter investigation of the accuracy of multidetector CT angiography alone and combined with venous-phase imaging (CT angiography-CT venography) for the diagnosis of acute pulmonary embolism.38Combined CT angiography-CT venography was found to have higher diagnostic sensitivity than CT angiography alone, but the increased diagnostic yield is probably not enough to justify the additional radiation.39 The predictive value of either approach is high when the result is concordant with clinical assessment, but clinicians should be wary and consider additional testing when results are discordant with clinical probability.38,39
Echocardiography is not a sensitive test for pulmonary embolism. Sonographic criteria for pulmonary embolism include right ventricular dilation, septal wall motion abnormality, decreased right ventricular contractility, elevated pulmonary artery or right ventricular pressures, moderate to severe tricuspid regurgitation, and visualization of the clot in the right ventricle or pulmonary artery. Sensitivity is only 41% and specificity is 91%.33,110
Magnetic
resonance imaging of the chest can be performed relatively rapidly, but
continues to have limited availability. The diagnostic performance of
MRI is similar to that for V/Q scanning. One advantage is that MRI does
not use ionizing radiation and therefore may be safer for imaging
pregnant patients.24
ACR's Appropriateness Criteria for CXR in uncomplicated asthma is only 4/9.4 A CXR is often recommended for the first episode of wheezing. Based on a retrospective review of 90 episodes of acute asthma in adults, Findley et al reported that the chest radiograph findings were most commonly normal (55%), hyperinflated (37%), or showed interstitial changes previously identified on radiographs (7%). Only one new alveolar infiltrate was found in this series (1%). They concluded that, in the setting of acute asthma, the chest radiograph is indicated only when pneumonia or pneumothorax is suspected.16 Abnormal CXR findings are more common in children with first episodes of wheezing (6 to 16%), but, in the absence of clinical variables, these findings rarely affect the acute management of the patient.17-19
Acute Exacerbation Of Chronic Obstructive Pulmonary Disease
Approximately one-fourth of radiographic abnormalities seen in patients with apparent exacerbations of chronic obstructive pulmonary disease are not predictable on the basis of high-risk criteria. Consequently, routine chest radiography should be considered.20 ACR's Appropriateness Criteria for uncomplicated COPD is 7/9; the appropriateness rating increases to 9/9 in the presence of leukocytosis, bandemia, chest pain, or cardiac history.4
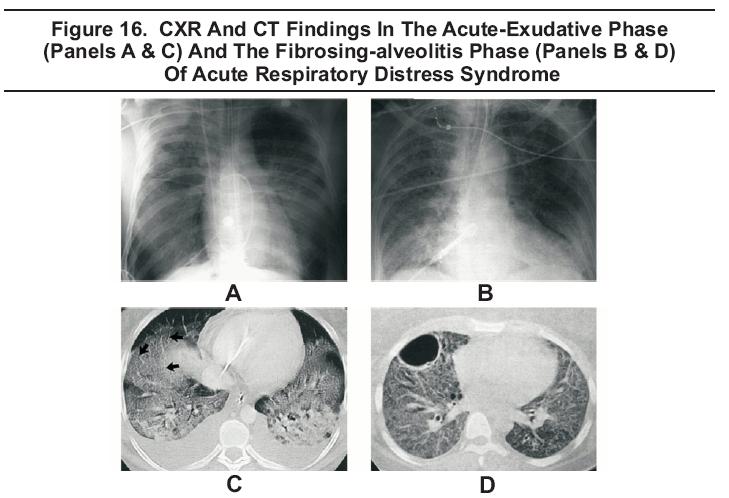
In the acute or exudative phase of acute respiratory distress syndrome (ARDS), CXR findings include bilateral, patchy, assymetrical pulmonary infiltrates. There may be associated pleural effusions (Figure 16 A). The pattern is indistinguishable from cardiogenic pulmonary edema.111 CT findings include alveolar filling, consolidation and atelectasis, predominantly independent lung zones (Figure 16 C). 112
In
the fibrosing alveolitis phase, the CXR shows linear opacities,
consistent with evolving fibrosis and possibly pneumothorax which is
seen in approximately 10% of cases (Figure 16 B). CT shows diffuse interstitial opacities and bullae (Figure 16 D).111,112 In the recovery phase, radiographic abnormalities resolve completely." 111,112
The CXR gets a relatively low ACR appropriateness rating (4/9) for adults less than 40 years of age with acute respiratory symptoms, negative physical examination, and no other signs, symptoms, or risk factors for pulmonary disease. The appropriateness rating goes up to 8 when the patient is greater than 40 years of age or has dementia, hemoptysis, leukocytosis, hypoxemia, or cardio-respiratory disease.4
The 2001 American Thoracic Society Guidelines lists the indications for CXR as newly acquired respiratory symptoms, such as cough, sputum production, dyspnea, associated fever, or auscultatory findings.9 For patients with advanced age113 or inadequate immune response, additional indications include confusion, failure to thrive, worsening of underlying illness, falls, and tachypnea114 .
The
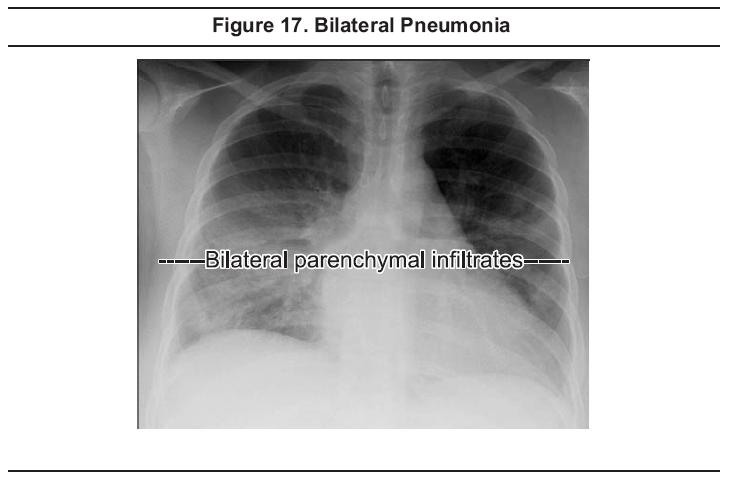
CXR may help to determine which patients should be hospitalized.
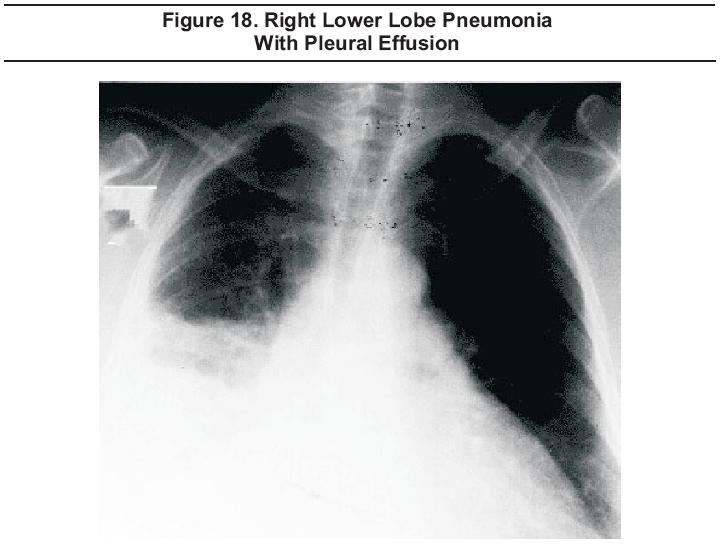
Admission is indicated when the CXR shows bilateral involvement (Figure
17), multilobar involvement, cavitation, rapid progression, or pleural
effusion (Figure 18). In addition, the CXR may help in differentiating pneumonia from other conditions, may
suggest specific etiologies, and may detect coexisting conditions, such
as lung abscess or bronchial obstruction.
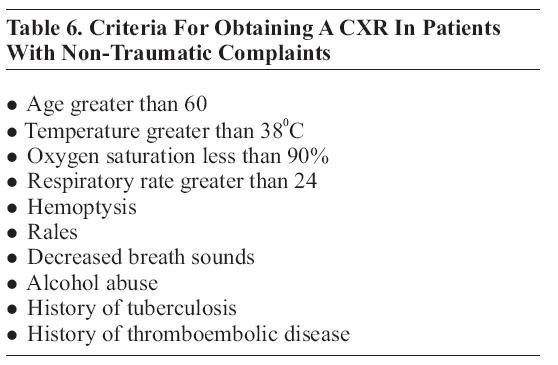
In 2002, Rothrock et al proposed a decision rule for when to obtain a CXR for non-traumatic presentations. They concluded that the presence of any of 10 criteria necessitates CXR and that, when used in this fashion, the CXR has a sensitivity of 95% and specificity of 40% for acute pulmonary pathology;11 see Table 6.
Emerman
et al found that physician judgment as to when to order a CXR
outperformed many decision rules with a sensitivityof 86% and a
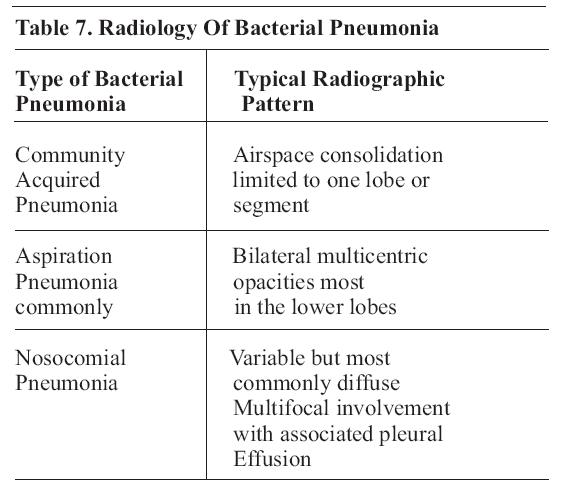
specificity of 58%.12 Traditional
classification of pneumonia into lobar and bronchial is less useful
than a moreclinical classification; see Table 7. 115
Chest radiography has traditionally been recommended as a part of the work up for febrile children (greater than 380C or 100.40 F) younger than three months. However, based on meta-analysis of three studies including a total of 617 infants, the chance of a positive chest radiograph in a febrile infant younger than three months of age with no pulmonary signs or symptoms was found to be only approximately 1%.10,13,14 For children older than three months of age, CXR should be considered for febrile children with temperature greater than 390 C or 102.2 0F and a WBC count greater than 20,000/mm . 3 15 CXR is usually not indicated in febrile children older than three months of age with temperature less than 390 C without clinical evidence of acute pulmonary disease.10
Chest radiograph cannot, by itself, be used to differentiate between viral and bacterial disease.116 Alveolar (lobar) infiltrate is an insensitive but reasonably specific indication of bacterial infection.116
ACR's Appropriate Criteria gives chest radiograph a highly appropriate (9/9) rating for the evaluation of HIV positive patients with cough, dyspnea, chest pain, or fever. CT of the chest is also appropriate (8/9) in HIV positive patients with acute respiratory symptoms and negative or non-specific CXR findings. If there is a high clinical suspicion for a pulmonary infection in the setting of a normal chest radiograph, a high-resolution, non-contrast CT scan may be warranted to assess for subtle abnormalities. Patients who have a normal chest radiograph and PCP will usually exhibit focal areas of ground-glass opacity on CT.5
CT is only moderately appropriate (4/9) when CXR shows diffuse infiltrates. It is highly appropriate (8/9) when non-infectious diseases are suspected. CT findings can frequently suggest the diagnosis, or at least limit the diagnostic possibilities, and may identify optimal sites for obtaining a biopsy.5
The radiological presentation of primary tuberculosis is variable. Parenchymal infiltrates anywhere in the lung fields are possible and pleural effusion may be associated or may occur alone. Hilar adenopathy is sometimes the only finding.117
The
typical radiological presentation of post-primary tuberculosis in
adults (reported in 58% of patients) is with infiltration nodules in
the upper zones, with or without cavitation (Figure 19).117 Pediatric
post-primary pulmonary tuberculosis typically shows consolidation,
cavitation, multi-focal ill-defined airspace opacities in the upper
lobes, apical pleural thickening, and evidence of prior pulmonary
tuberculosis.118

Screening chest radiography is indicated for patients with positive screening tests but need not include lateral views. Meyer et al compared PA CXR with PA and lateral CXR in 535 cases and found that the lateral view identified findings not present on the PA view in only 0.4% cases, and in no case did the unique findings on the lateral view alter patient management.119 High resolution CT has been used to predict activity.120
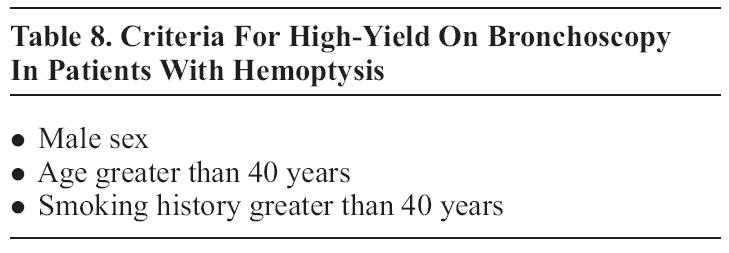
Chest radiography should be included in the initial evaluation of patients presenting with hemoptysis.121 Based
on a retrospective review of records of 119 bronchoscopies performed
for hemoptysis, O'Neil et al concluded that patients with less than two
risk factors for malignancy and negative CXR may be managed with
observation; see Table 8.121CT and bronchoscopy are complementary examinations in patients with two
or more risk factors for malignancy or with persistent/recurrent
hemoptysis and negative CXR.122 ACR's Appropriateness Criteria for CT in this setting is
high at 8/9.6 In patients with two or more risk factors for malignancy
and positive chest radiograph, ACR's Appropriateness Criteria for CT is
also 8/9.6
CT may be better than bronchoscopy at defining the cause of hemoptysis; the two modalities are equally effective at determining the site of bleeding.123
Massive
hemoptysis (greater than 300 mL/24 hrs) can be effectively treated with
either surgery or percutaneous bronchial artery embolization.124 Embolization for massive hemoptysis receives an ACR appropriateness rating of 8/9.6
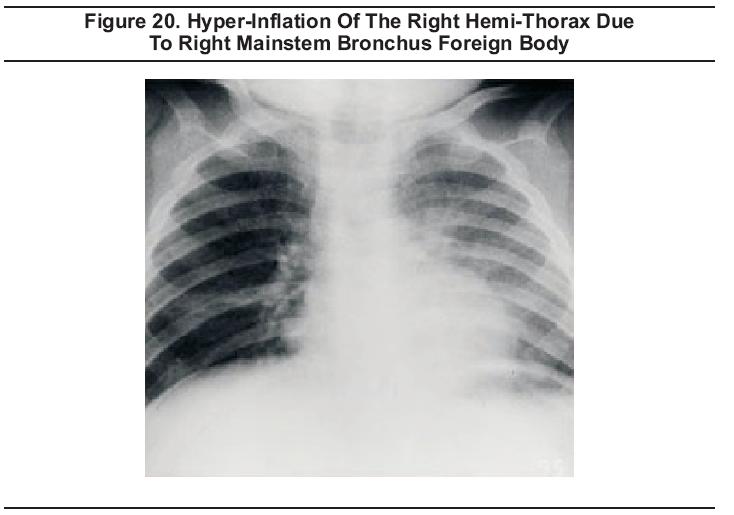
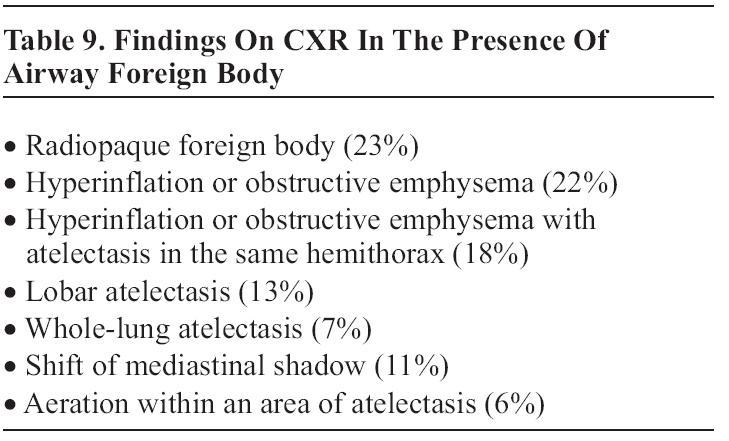
Chest radiograph findings in the presence of an airway foreign body
(Figure 20) based on a retrospective chart review of 133 children are
shown in Table 9.125
Non-contrast CT is easy, fast, and 100% sensitive for upper esophageal foreign bodies.126It should be the first choice for diagnostic imaging of suspected upper esophageal foreign bodies not expected to be visible on plain radiographs. CT may also detect foreign bodies not seen with barium studies.126
Acute Coronary Syndromes/Acute Myocardial InfarctionEchocardiography (ECHO) may be used to evaluate for wall motion abnormalities and is frequently included as a part of an emergency cardiology consultation. ECHO may also be used as an adjunct to exercise or pharmacological stress testing. The American College of Cardiology, the American Heart Association, and the American Society of Echocardiography have issued joint guidelines for clinical use.40
While there are a wide array of class I and IIa indications for adult and pediatric cardiology patients, those
most pertinent for emergency department patients have to do with the
evaluation of chest pain patients and establishing the diagnosis and
prognosis of chronic ischemic heart disease. Per the ACC/AHA/ASE
guidelines, ECHO is a class I recommendation for the evaluation of
chest pain in patients with suspected acute myocardial ischemia when
baseline ECG and laboratory markers are non-diagnostic and when the
study can be obtained during pain or within minutes after its
abatement. The use of ECHO in this way, however, generally requires the
physical presence of a cardiologist trained in the use of ECHO for the
detection of wall motion abnormalities early in the course of the
event, which is not achievable in many centers. ECHO is not indicated
for chest pain of apparent non-cardiac etiology nor is ECHO indicated
for patients who have electrocardiographic changes diagnostic of
myocardial ischemia/infarction.40
ECHO is also indicated for patients with chest pain who have
hemodynamic instability or who are suspected of having valvular,
pericardial, or aortic disease.40
Exercise or pharmacological stress ECHO is recommended as a class I intervention for the diagnosis of myocardial ischemia in symptomatic individuals or for selected patients in whom the ECG assessment is less reliable. These patients include those with intermediate pretest likelihood of coronary artery disease and digoxin use, left ventricular hypertrophy (LVH) of 1 mm or more of ST depression at rest, pre-excitation syndrome, or complete left bundle branch block (LBBB). Exercise echocardiography is also recommended at the class IIa level for the detection of myocardial ischemia in women with a low or intermediate pretest likelihood of coronary artery disease. ECHO is not indicated for the screening of asymptomatic patients with a low likelihood of coronary artery disease or as routine periodic reassessment for stable patients. Stress ECHO should not be used as a routine substitution for treadmill exercise testing in patients for whom ECG analysis is expected to suffice.40
A
meta-analysis based on three studies of rest echocardiography used to
assess for acute cardiac ischemia in the ED setting reported that
sensitivity was excellent at 93% and specificity was rated as good at
66%.127 A
subsequent report in 2002 cited the sensitivity at 91%, but noted that
false negative studies may be associated with small MI's.128
Cardiac Arrest: In the setting of cardiac arrest, echocardiography can be used for the detection of cardiac motion. Patients without cardiac activity do not survive regardless of electrical activity.129,130 Echocardiography may also be used to evaluate for tamponade as a cause for pulseless electrical activity.130 Pericardial tamponade and electromechanical dissociation are truly emergent and potentially lethal cardiovascular conditions requiring emergency diagnosis.99
Nuclear Medicine Scanning: Both thallium-201 and technetium-99m radiopharmaceuticals are commonly
used for myocardial scanning with imaging using single photon emission
computed tomography (SPECT). Several technetium-99m labeled agents are
available but the most used and studied is sestamibi.131
The ACC/AHA/ASNC Guidelines for clinical use of cardiac radionuclide imaging recommend cardiac stress myocardial perfusion SPECT at the class I level in order to identify the extent, severity, and location of ischemia in patients who are able to exercise and who have a baseline ECG abnormality that interferes with the interpretation of exercise-induced ST-segment changes, i.e., pre-excitation syndromes, LVH, digoxin therapy, or greater than 1 mm ST depression. Adenosine or dipyridamole myocardial perfusion SPECT is recommended in patients with left bundle branch block or electronically-paced ventricular rhythms and for those patients unable to exercise. The use of exercise myocardial perfusion SPECT as the initial test for patients who are considered to be at high risk (e.g., diabetics) is given a class IIa recommendation.41
The diagnostic accuracy of rest myocardial perfusion imaging in patients who have acute chest pain and normal or non-diagnostic ECGs has been found to be high. Based on eight studies between 1979 and 2002, sensitivity was reported to be 90 to 100%, specificity 60 to 92%, and negative predictive value 99 to 100%.132Studies performed in lower-risk patients have demonstrated that emergency department perfusion imaging does offer incremental value. In a large, prospective, randomized, controlled study, 2475 patients were randomized to routine care or to routine care with myocardial perfusion imaging. A significantly lower admission rate was achieved in the imaging group without reducing appropriate admission for patients with acute ischemia.133Nevertheless, there are several problems that limit the use of myocardial perfusion imaging. First, there are some technical problems in obtaining high quality images that allow differentiation of diaphragm and breast shadows from pathologic perfusion defects. Second, detection of new perfusion defects is complicated in patients with previous myocardial infarction. In many centers, availability of the test is limited to certain hours of the day, and the lack of availability of experienced readers may limit the usefulness of the scans. Finally, there continues to be some controversy over whether the injection of radioactive tracers must be performed while the patient is experiencing ischemic symptoms or whether the injection may occur soon after symptom resolution.134
Exercise
SPECT myocardial perfusion imaging is preferred in patients with
greater than 1 mm ST depression or pre-excitation syndrome on their
resting ECG, as well as for those who have undergone percutaneous
transluminal coronary angioplasty (PTCA) or coronary artery bypass
grafting (CABG).131 In addition, patients with less than 1 mm ST depression on
their resting ECG, those on digoxin, and those with LVH, LBBB, and
ventricular pacing may be considered for SPECT myocardial perfusion
imaging.131
Echocardiography
performed by emergency physicians has been shown to be a reliable
technique for evaluating suspected pericardial effusions (Figure 5).
In a study of 515 high-risk patients with images captured on video and
subsequently reviewed by cardiologists, emergency physicians detected
pericardial effusion with a sensitivity of 96% and a specificity of 98%.136ECHO has been suggested for use in further evaluating ED patients
presenting with a complaint of dyspnea but for whom no cause has been
found after standard ED evaluation. In a prospective observational
study of 103 patients who presented with new-onset dyspnea but lacked
any pulmonary, infectious, hematological, traumatic, psychiatric,
cardiovascular, or neuromuscular explanation for their dyspnea after ED
evaluation, Blaivas found a 14% incidence of pericardial effusion and
recommended the use of bedside ultrasound in the evaluation of such
patients.137
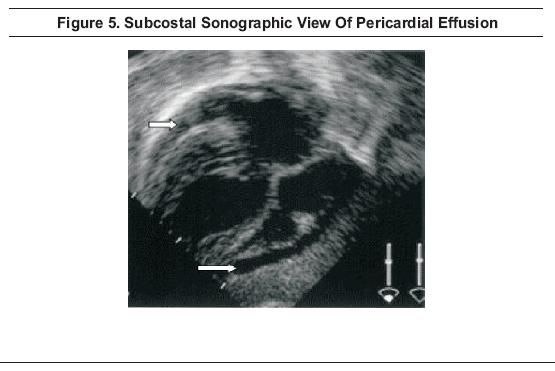
Pericardial effusion appears as a dark band between the pericardium and myocardium on sub-costal view (Figure 5). Evaluation for tamponade is accomplished by looking for "swinging heart sign," right ventricular collapse during mid-late diastole, or inferior vena cava plethora.
Echocardiographic
guidance for drainage of pericardial fluid is the standard of care and
has a 97 to 100% success rate with a complication rate of 5% and a
major complication rate of 1.2%; the most commonly reported
complications are hemothorax and infection.100,138 The
use of a pericardial catheter for extended drainage has become more
common, with a concomitant reduction in the rate of recurrence and
subsequent pericardial surgery.138
In patients suspected of having infective endocarditis, the diagnosis can be facilitated by the identification of vegetations on heart valves. Echocardiography has therefore assumed a vital role in the diagnosis of this disorder. The Duke Criteria has improved the specificity and sensitivity of the diagnosis of infective endocarditis by assigning major and minor criteria, including echocardiographic findings of an oscillating intracardiac mass or vegetation, an annular abscess or new valvular regurgitation, or prosthetic valve partial dehiscence.40,139
While both TTE and TEE can identify valvular vegetations, TEE can identify much smaller vegetations and has significantly greater sensitivity, 44% and 94% respectively. Specificity is similar for the two techniques at 98% and 100% respectively.140 When the diagnosis of infective endocarditis is suspected, obtain prompt cardiology consultation. Transthoracic ECHO may be used as the initial screening test, followed by TEE if the results are negative or equivocal.50
Spontaneous Aortic Dissection And Hemomediastinum
Chest
radiograph findings of hemomediastinum include widened mediastinum
(greater than 8 cm at aortic arch in the supine position), blurred
aortic knob (Figure 12),
left apical pleural cap, opacified aorticopulmonary window, widened
right paratracheal stripe (greater than 4 mm), and left pleural
effusion. Additionally, the calcium sign, consisting of a discontinuity
of the calcification within the aortic knob or a separation of the
calcified intima from the outer aortic border of greater than 1 cm,
suggests dissection.

Chest
radiograph findings are usually abnormal in the presence of aortic
dissection and CXR has a reported sensitivity of 90%. The presence of a
normal aorta and mediastinum on CXR decreases the probability of
dissection, but does not exclude it. The negative likelihood ratio is
0.3.141Positive findings include change in aortic silhouette, widening
(especially if progressive compared to old films), indistinct contour
or blurred aortic knob, irregularity and separation of outer vessel
wall, and intimal calcium (Figure 21).
In addition, displacement of adjacent structures may be seen as the
esophagus with nasogastric tube to the right and posterior, trachea to
the right and anterior, or left mainstem bronchus inferiorly.141

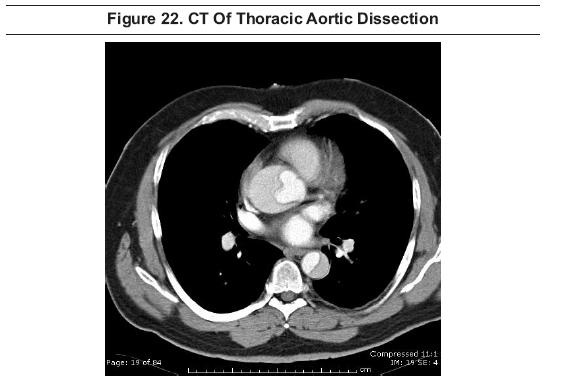
The contrast-enhanced multi-slice CT scan has become a standard test for aortic dissection.21 In fact, multi-slice CT scanning now appears to be the modality of choice for complete examination of the entire aorta.22 Computerized
tomography provides excellent visualization of the aorta and branch
vessels and their relationship to surrounding structures (Figure
22).21,22 Contrast is required to optimally depict the vessel lumen.51
The sensitivities of TEE, CT, and MRI for detecting dissection are similar at about 98%. TEE may provide more information on detailed anatomy of the valves in the setting of proximal dissection, and can provide functional data on regurgitation that CT cannot. By contrast, the sensitivity for TTE is only 59%.51 Specificities are 77% for TEE, 83% for TTE, 87% for CT, and 98% for MRI. CT was reported to be less effective in detecting an entry site or aortic regurgitation. Based on these findings, a noninvasive diagnostic strategy of using MRI in hemodynamically stable patients and TEE in unstable patients has been proposed.51
MRI provides at least equivalent visualization to CT and can be effectively used with or without contrast. Drawbacks include the lack of availability or poor accessibility in the emergency situation and difficulty in visualizing distal branch vessels. However, the use of MRI may obviate the need for conventional angiography in some cases.51,52
Chest
radiography usually shows widening of the mediastinum, enlargement of
the aortic knob, tortuosity, calcification, or tracheal deviation when
there is aneurysmal dilatation of the thoracic aorta, but actual size is difficult to assess (Figure 12).142,143 However, the chest radiograph can be completely normal.144If the chest film shows abnormalities consistent with thoracic aortic
aneurysm, one should have a low threshold for ordering a
contrast-enhanced CT scan to better define the aortic anatomy.142,143
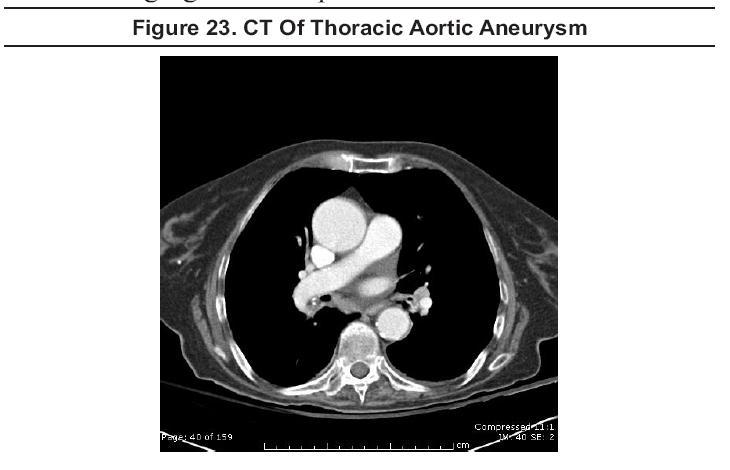
Contrast-enhanced CT scanning (Figure 23)
and magnetic resonance angiography (MRA) are the preferred modalities
to define aortic (and branch vessel) anatomy, and both accurately
detect and size thoracic aortic aneurysms. When aneurysms involve the
aortic root, MRA is preferable since CT images the root less well and
is less accurate in sizing its diameter.142,143
Transthoracic
echocardiography is effective for imaging the aortic root, but it does
not consistently visualize the mid or distal ascending aorta or the
descending aorta. TTE should generally not be used for diagnosing or
sizing thoracic aortic aneurysms. TEE can visualize the entire thoracic
aorta well, but, due to its semi-invasive nature, it is generally not favored for routine imaging of stable patients.143
Congestive Heart Failure/Pulmonary Edema
The chest radiograph (Figure 24)
is rated as highly appropriate (9/9) when new onset heart failure (HF)
is suspected based on symptoms and physical examination, and is rated
as highly appropriate (9/9) with previously diagnosed HF and new or
worsening symptoms. CXR is less appropriate (4/9) for patients with
previously diagnosed HF and stable symptoms.8

Based on the analysis of the Acute Heart Failure National Registry (ADHERE) database, Collins et al reported that nearly 20% of patients admitted to the ED with acutely decompensated heart failure (ADHF) showed no signs of pulmonary congestion on chest radiography and suggested that clinicians not rule out heart failure in patients with no radiographic signs of congestion.144 While the initial ED CXR may be insensitive in predicting a hospital discharge diagnosis of ADHF, CXR is a simple test that remains helpful in the diagnosis of the majority of patients with ADHF and in establishing alternative diagnoses in many others.145
Congestive
heart failure is readily diagnosed on CT obtained for other
indications, but symptoms of congestive heart failure do not, of
themselves, provide a sufficient indication for CT scanning (ACR
appropriateness rating: 2/9). 8
Gary R Strange; Bruce MacKenzie
November 1, 2006
Wrist Injuries Emergency Imaging And Management
Emergency Imaging For The 21st Century: Where Does Ultrasound Fit In?
An Evidence-Based Approach To Imaging Of Acute Neurological Conditions
Imaging In The Adult Patient With Nontraumatic Abdominal Pain
Accredited By





Our Partners

