The most commonly ordered imaging study of the thorax remains the chest radiograph (CXR) with routine studies including the posteroanterior (PA) and lateral views. Patients who cannot be transported to the radiology suite are often studied using a portable anteroposterior (AP) view.
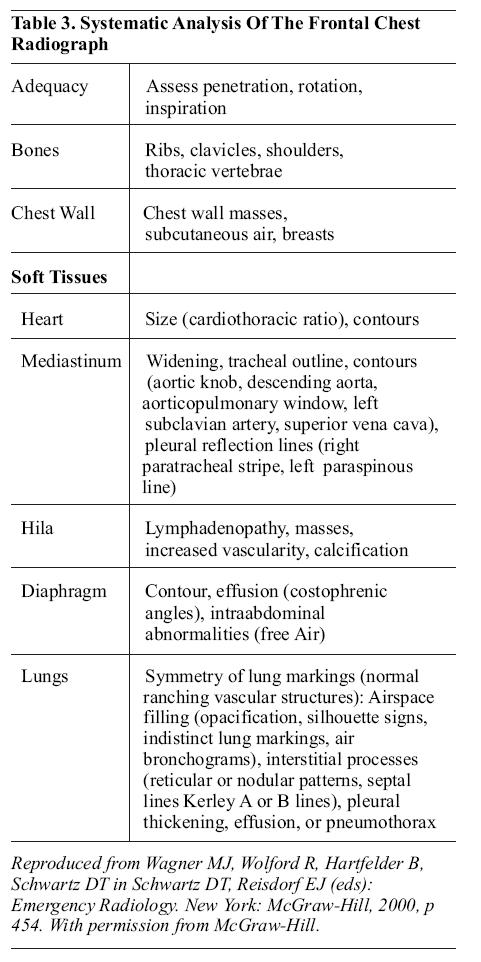
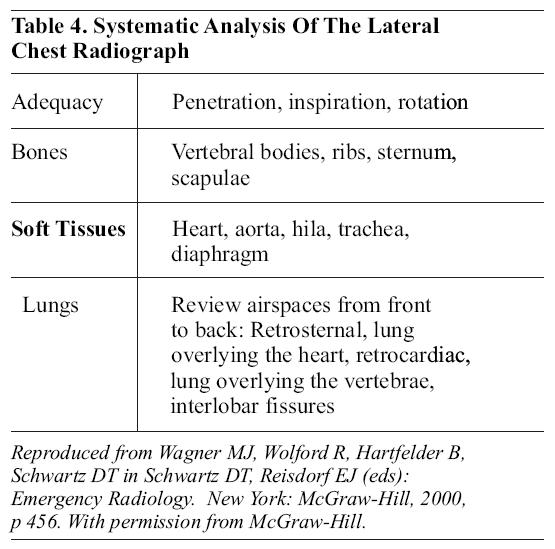
General guidelines for the interpretation of chest radiographs have been well-outlined by Schwartz et al;59,60 see Tables 3 and 4.
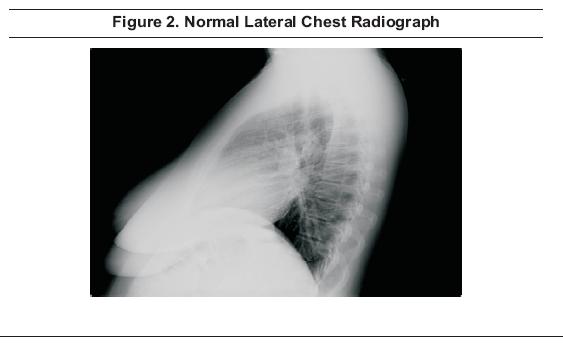
In the interpretation of the lateral PA and AP chest (Figures 1 and 2 ),
the first concern is to assure the adequacy of the film. The entire
thorax should be seen, including the apices, lateral chest walls,
entire diaphragm, and both costophrenic angles.

Penetration
should be such that the lower thoracic vertebral bodies are faintly
visible behind the heart and the image should be positioned so that the
mid-point between the clavicular heads is superimposed over the spinous
processes of the thoracic vertebrae. The film should be shot in
inspiration so that the right costophrenic sulcus is below the
posterior costovertebral junction of the 10th rib.
Systematic analysis of the images begins with the assessment of the bony thorax, including the ribs, clavicles, shoulders, and thoracic vertebral bodies.
Heart size is considered normal if the cardiothoracic ratio is less than 0.5; cardiomegaly is present if the cardiothoracic ratio is greater than 0.5. Thoracic width is measured at the widest point, i.e., the lung base. The cardiac contours are assessed for evidence of chamber enlargement.
Mediastinal widening is present when the mediastinum measures greater than 8 cm at the aortic arch in adults or the mediastinum:chest width ratio is greater than 0.25 in children. The trachea should be in the midline. The contours of the mediastinum are assessed, noting the aortic knob, descending aorta, aorticopulmonary window, left subclavian artery, superior vena cava, right paratracheal stripe, and left paraspinous line.
The hila of the lungs are assessed looking for adenopathy, masses, vascularity, and calcifications.
The diaphragm is evaluated looking at the contour, costophrenic sulci, and for any evidence of free air in the space beneath the diaphragm.
The lungs are evaluated for symmetry. Lung markings should be visible as a branching vascular pattern. The air spaces are evaluated for evidence of opacification, silhouette signs, or air bronchograms. The retrosternal space, retrocardiac space, and interlobar fissures are assessed. Interstitial processes may be detected as a reticular pattern, a nodular pattern, or as septal lines (Kerley A or B lines).
The pleura may show thickening or the pleural space may contain fluid (effusion) or air (pneumothorax).
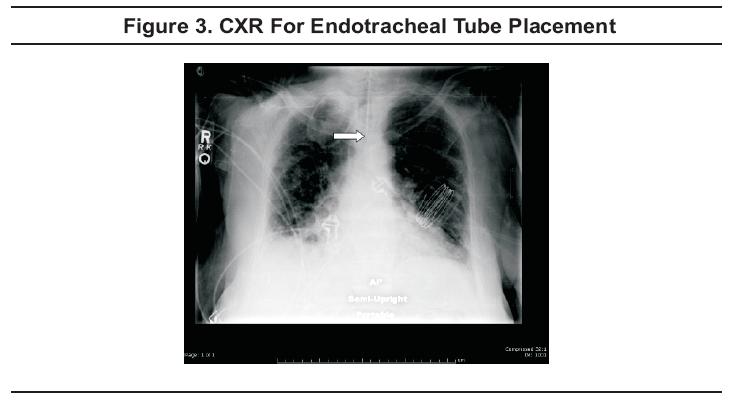
The CXR is an essential part of the assessment of endotracheal tube placement (Figure 3).
The preferred location is 3 to 4 cm above the carina. In addition, the
CXR may exclude pneumothorax and can potentially confirm various
diagnoses, such as pneumonia or congestive heart failure.61
Central Line Placement
Ultrasound guidance of central line placement may decrease the time required and the number of attempts necessary prior to successful cannulation.62However, while it has the potential to improve successful line placement and to minimize complications, such a reduction in complication rate has yet to be confirmed.63,64
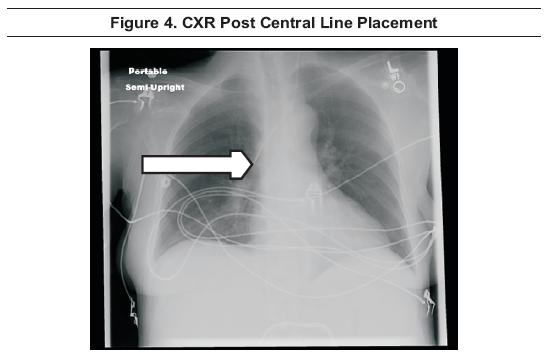
A
chest radiograph has long been recommended following any attempt at
placement of a cervical or thoracic central line. CXR allows for the
assessment of the location of the tip of the catheter (Figure 4) and
assists in ruling out pneumothorax or hemothorax, although supine films
are of limited value in assessing for pneumothorax or hemothorax due to
anterior layering of air and/or posterior layering of blood in these
views. However, confirmatory radiographs may not be needed after
straight-forward placements.65
Gary R Strange; Bruce MacKenzie
November 1, 2006
Wrist Injuries Emergency Imaging And Management
Emergency Imaging For The 21st Century: Where Does Ultrasound Fit In?
An Evidence-Based Approach To Imaging Of Acute Neurological Conditions
Imaging In The Adult Patient With Nontraumatic Abdominal Pain
Accredited By





Our Partners

