About This Course
Syncope is the transient loss of consciousness and postural tone, with spontaneous recovery. It accounts for approximately 1% of all emergency department visits. Postsyncopal patients often present to UC and primary care offices after the event, so even nonemergency clinicians must have a systematic, evidence-based approach to evaluate the syncopal patient. In a very small subset of patients, syncope may be a warning sign for serious outcomes or death, but identifying these patients is challenging, as the clinician must distinguish between life-threatening causes and the more common, benign etiologies. Research on syncope is often observational, and clinical decision rules frequently perform poorly in validation studies. This lack of data leads clinicians to transfer many syncopal patients with benign presentations to the ED. This course reviews the useful clinical and diagnostic findings for safely and efficiently risk-stratifying patients presenting to UC with syncope.
What are the key features that distinguish high-risk syncope from low-risk syncope?
Are risk-stratification tools helpful, and when should they be used?
When is ED transfer appropriate?
Case Presentations
- History reveals that the patient was getting a flu shot at a local pharmacy when she became lightheaded and diaphoretic and passed out, without striking her head.
- She was unconscious less than 1 minute and awoke with no confusion.
- Because she passed out, the pharmacist told the parents that they should “go immediately to UC” for evaluation…
- His wife tells you that the man lost consciousness while sitting in a chair. She states that he had generalized jerking of his extremities. He had a prompt return to normal level of consciousness, but was complaining of chest pain and shortness of breath after the event.
- The patient says that he underwent elective cholecystectomy 3 weeks ago, but denies abdominal pain or vomiting, and he says he has no other medical problems.
- His vital signs are: blood pressure, 96/54 mm Hg; heart rate, 122 beats/min; respiratory rate, 24 breaths/min; temperature, 37°C; and oxygen saturation, 92%.
- You wonder what this patient’s major underlying problem is…
- The patient states she was walking to the bathroom when she found herself on the floor with right knee pain, and no recollection of how she got there. She currently has no other complaints.
- Her vital signs are normal, and her past medical history is significant for diabetes and hypertension.
- You wonder if a right knee x-ray is all that’s indicated in this case…
Introduction
Resulting from global cerebral hypoperfusion, syncope is a transient loss of consciousness (TLOC), typically with associated loss of postural tone, followed by complete, spontaneous recovery. Syncope represents approximately 1% of all emergency department (ED) visits in the United States,1 but data on urgent care (UC) visits for syncope are incomplete. Annual expenditures for hospital admissions related to syncope are estimated at up to $5.6 billion in the United States.2 For most patients with syncope, hospitalization has a much smaller impact on mortality than the patient’s underlying morbidities.3
The primary task of the UC clinician is to distinguish syncope as a presentation of ongoing, life-threatening disease (such as subarachnoid hemorrhage, pulmonary embolism, and hypovolemia secondary to bleeding) from syncope that results from benign causes (such as vasovagal syncope), and from high-risk causes that may have resolved at the time of clinic presentation (particularly arrhythmias).4 The most effective tools for evaluating syncope remain the history, physical examination, and electrocardiogram (ECG), as advanced studies have shown vanishingly low yield for most patients with normal examinations and ECGs.5-10 Several clinical decision rules exist, but their utility has been questioned.11,12 This issue of Evidence-Based Urgent Care discusses the best available evidence to identify which patients with syncope can be safely discharged with limited testing, and which patients may benefit from further investigation, including ED transfer.
Etiology and Pathophysiology
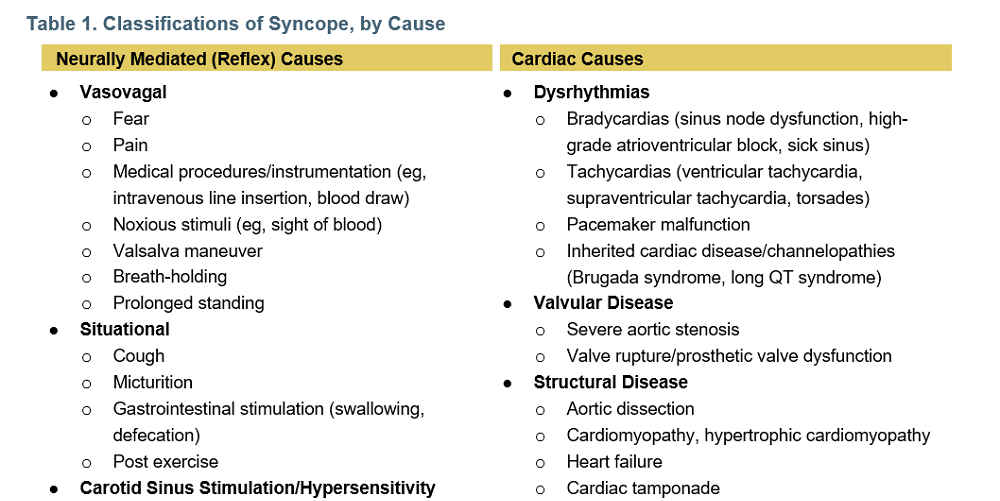
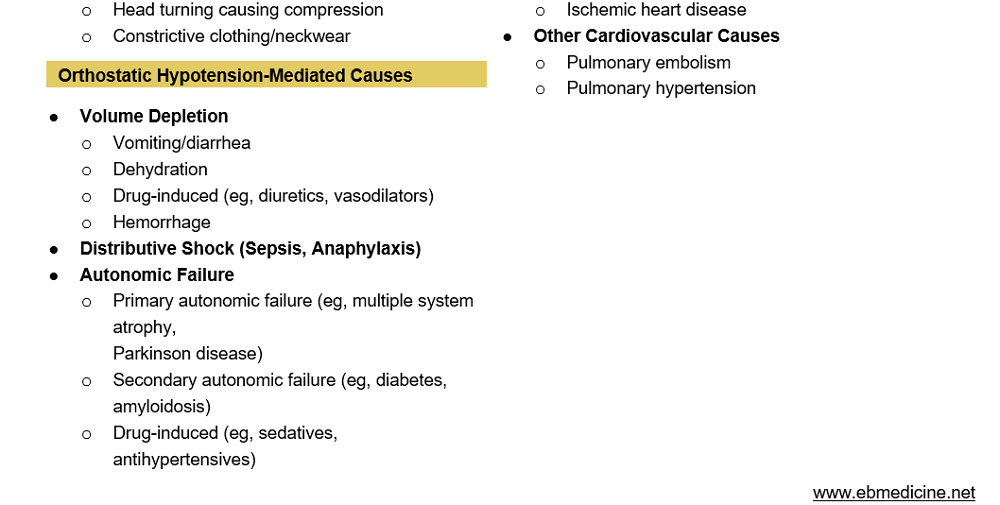
Syncope is a transient loss of consciousness (TLOC) that represents the final common pathway of several conditions causing hypoperfusion of the brain. This hypoperfusion may result from decreased peripheral vascular resistance, decreased cardiac output, or both, and is commonly divided into 3 classifications: (1) neurally mediated (reflex) syncope, (2) orthostatic hypotension, and (3) cardiac syncope. These categories can be subdivided, as noted in Table 1. Although no cause is identified in the majority of patients, neurally mediated syncope is the most common cause of syncope identified, followed by orthostatic syncope, and then cardiac syncope.13 Syncope is most commonly a benign diagnosis, with a review of 22,189 patients finding a 30-day risk of death in patients aged <60 years without a history of heart failure to be 0.2%.14 A meta-analysis of 43,315 patients found a 4.4% risk of death (95% confidence interval; 3.1%–5.1%) for all ED patients with syncope, with 1.1% due to a cardiovascular etiology. Palpitations preceding syncope, exertional syncope, and a history of heart disease (especially heart failure) were the most powerful predictors of adverse outcomes.15
Having defined syncope as a transient state of global cerebral hypoperfusion, it is not a great leap to assert that a transient decrease in blood pressure is the most basic physiologic explanation. Cardiovascular physiology gives us this central principle and formula:
MAP = CO × SVR
MAP = Mean arterial pressure
CO = Cardiac output
SVR = Systemic vascular resistance
Breaking down cardiac output into its components yields this:
MAP = (HR × SV) × SVR
HR = Heart rate
SV = Stroke volume
In the case of syncope (and shock), it is frequently helpful to determine which of the variable(s) on the right side of the equation could be responsible for the patient’s decrease in MAP. A decrease in any of the variables on the right side of the equation brings a concurrent decrease in MAP. For example, bradyarrhythmias decrease cardiac output by decreasing heart rate; dehydration and blood loss decrease cardiac output by decreasing stroke volume; and anaphylaxis comes with a massive drop in SVR. Increased vagal tone can cause a decrease in all 3 of the variables on the right side of the equation. This principle makes intuitive sense until one considers the extreme tachycardias. Tachycardia is a compensatory mechanism in shock, but inappropriate tachycardia brought on by dysrhythmia (for example, ventricular tachycardia) can literally lead to diminishing returns. If the heart rate is so fast that the left ventricle cannot adequately fill, the resultant decrease in stroke volume will actually bring a drop in MAP.
The human autonomic nervous system has the ability to adjust 1 or more of the variables on the right side of the equation nearly instantly and reflexively in response to a pathologic change in one of the others. Syncope itself can be viewed as a protective phenomenon that serves to correct inadequate oxygen and glucose delivery to the brain; when the subconscious brain is not getting what it needs, it demands that the body go horizontal to make the job of the heart easier.
Neurally Mediated Syncope
Neurally mediated syncope may result from inappropriate bradycardia, decreased vasomotor tone, or both, and is more common in those younger than 40 years. Younger people are more likely to have typical prodromal symptoms, such as nausea and sweating, than older adults.16 Vasovagal syncope is frequently triggered by pain or intense emotions, and can be provoked by medical procedures and the sight of blood. Situational syncope is associated with increased vagal tone secondary to particular actions, including Valsalva maneuvers, following exercise, and occasionally gastrointestinal stimulation such as swallowing or defecation. Carotid sinus syncope may be induced from pressure on the carotid sinus such as head turning or shaving. Neurally mediated syncope is commonly recurrent and is associated with a good long-term prognosis.17
Orthostatic Hypotension-Mediated Syncope
Orthostatic hypotension is defined as a fall in the systolic blood pressure of >20 mm Hg upon standing, or symptoms such as dizziness. It results from volume depletion or autonomic failure, which is the inability of the sympathetic nervous system to increase vascular tone with changes in posture. Drug-related hypotension is the most frequent cause, although patients with orthostatic hypotension are usually older and have multiple comorbidities.18 Orthostasis may cause syncope by itself, or it may be incidentally present in other, more concerning causes. One study found no difference in 30-day serious outcomes between elderly patients with normal orthostatic vital signs and those with abnormal orthostatic vital signs.19 Be wary of diagnosing otherwise high-risk syncopal patients with benign orthostasis based on vital signs alone.
Cardiac Syncope
Cardiac syncope carries the highest morbidity of all causes, and patients with underlying cardiac disease who experience syncope have higher all-cause rates of mortality.20 Cardiac syncope may result from absent or ineffective contractions due to obstruction of blood flow (as with pulmonary embolism, aortic stenosis, and aortic dissection), or it may result from dysrhythmias. Dysrhythmias are the most common causes of cardiac syncope and may be challenging to diagnose, as they will most likely have resolved by the time of UC evaluation. A careful history and review of the ECG may provide some clues to an underlying etiology. Obstructive or structural causes of cardiac syncope will typically persist through the UC evaluation and are more easily identified.
Differential Diagnosis
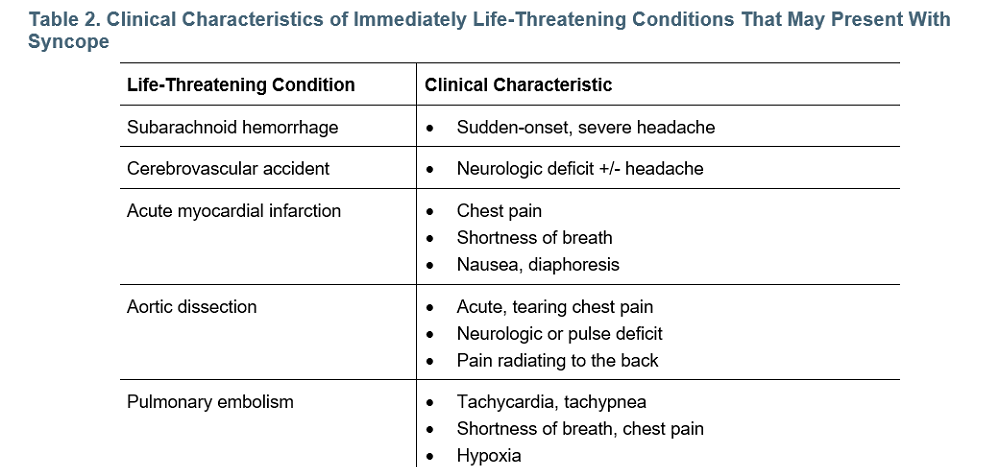
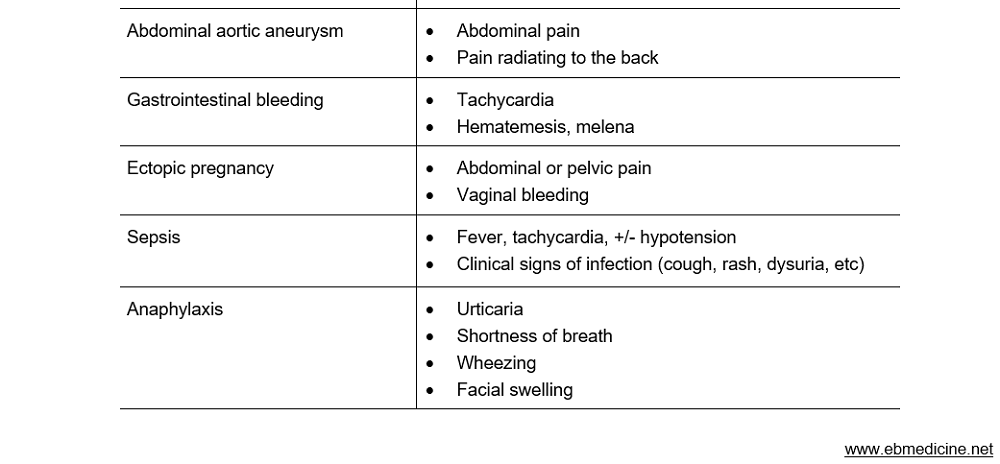
Any patient with neurologic deficit, headache, chest pain, abdominal pain, or persistently abnormal vital signs should not be diagnosed with isolated, benign syncope unless more serious diagnoses are excluded. See Table 2, for clinical findings that suggest a life-threatening etiology; note that all have presenting features other than isolated TLOC.
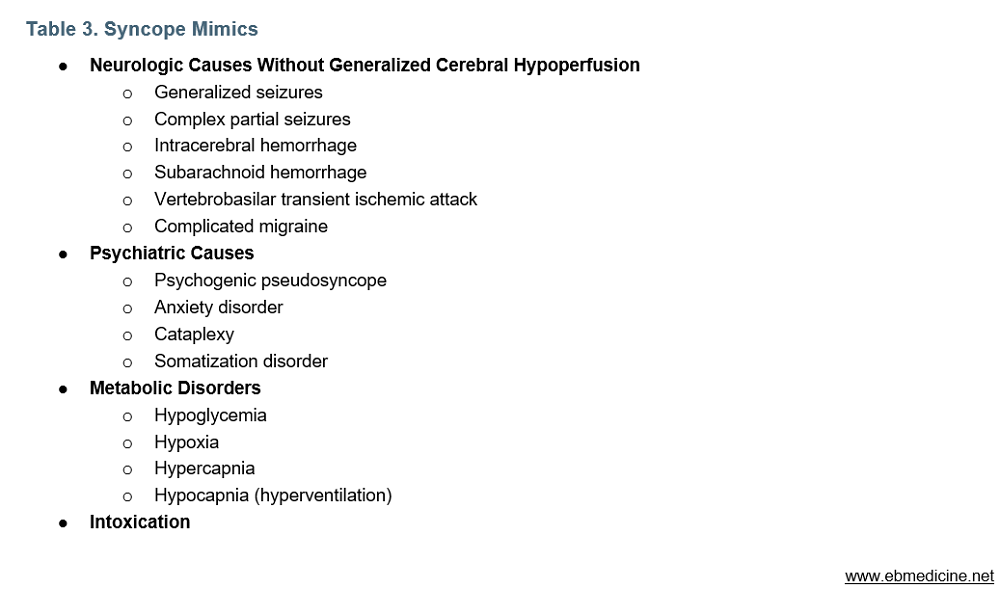
In patients for whom a life-threatening etiology is not apparent, the history is most helpful in distinguishing between syncope, seizure, psychogenic causes of TLOC, and rare causes of TLOC such as posterior circulation transient ischemic attack. Metabolic causes such as hypoglycemia and certain toxins or overdoses may result in TLOC, but they generally do not resolve spontaneously. Medications may cause orthostatic hypotension or prolonged QT intervals. See Table 3, for a list of syncope mimics; note that most of these do not rapidly resolve without intervention.
Seizure
It may be challenging to differentiate seizure from syncope, as both bring TLOC with subsequent full return to neurologic baseline. In addition, syncope may be accompanied by myoclonic convulsive activity. The most helpful feature indicating seizure is the presence of disorientation lasting more than a few seconds following the event.21,22 Other features that point toward seizure include tongue laceration, head-turning, and unusual posturing. Features more indicative of syncope include any presyncope (light-headedness, or palpitations), loss of consciousness with prolonged standing or sitting, and diaphoresis before the spell.23 Urinary incontinence cannot be used to reliably distinguish between seizure and non-seizure causes of TLOC.24 In general, seizure becomes a more likely etiology if >10 myoclonic jerks are witnessed.
Urgent Care Evaluation
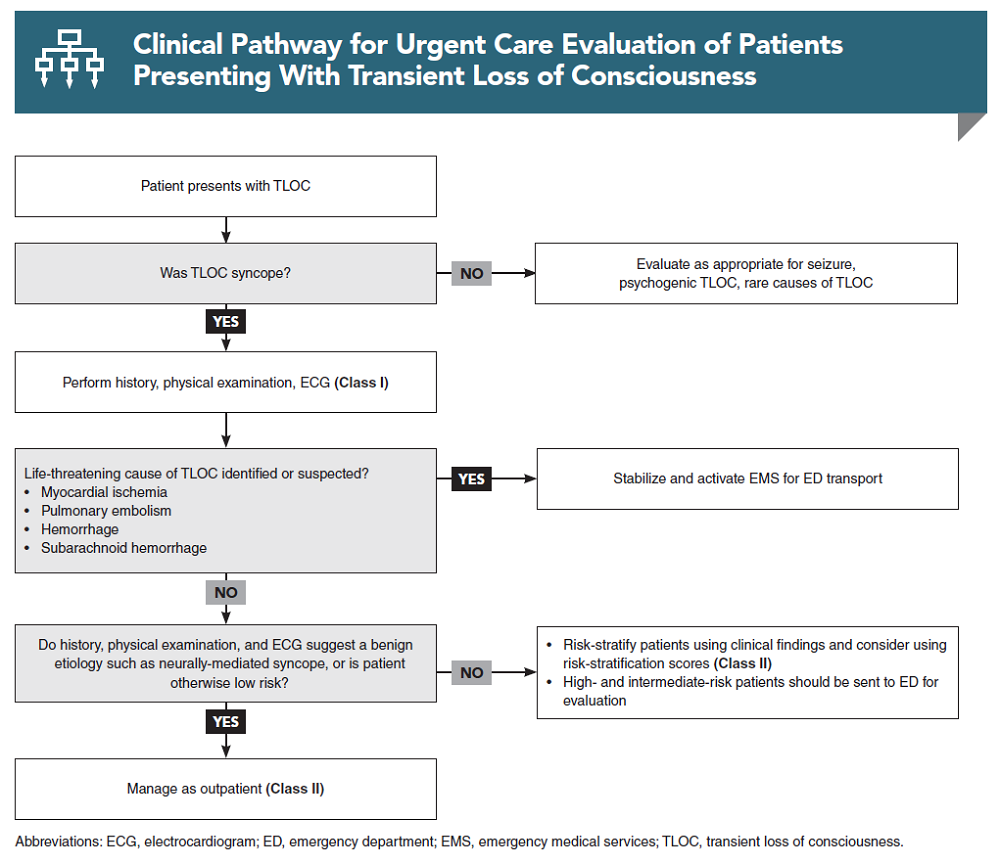
In evaluating the patient who presents to UC with TLOC, the clinician must first determine whether syncope is the predominant reason for the patient’s presentation or whether it is a symptom of a more serious underlying condition. If the presence of an immediate threat to life is determined, then stabilization and EMS activation should occur without delay. Otherwise, the focus shifts to accurately identifying syncope and classifying its etiology. As above, in many instances a clear etiology will not be quickly or easily identified. If no immediate life threats are present, the clinician should attempt to risk-stratify the patient to determine the appropriate disposition and follow-up plan.
History
The importance of the history of present illness in syncopal patients cannot be overstated.25 Inquire specifically about activity and symptoms immediately before the event, as well as during and after the loss of consciousness, and try to elicit information such as the patient’s position (standing, sitting, or changing position), environment, prodrome, palpitations, exertion, and duration. Symptoms such as chest pain, shortness of breath, headache, and neurological deficit should be noted. Syncope without prodrome may be more likely to be caused by arrhythmias.26
Ask whether the patient has a history of passing out or fainting, and if they do, whether this episode differs from previous episodes. Recurrent syncope is common but does not appear to be a significant predictor of mortality.27,28 In particular, vasovagal syncope often has known triggers.29 Inquire about any previous treatment or evaluation, including cardiac monitoring. Falls without a clear mechanism should be considered as potential syncopal events, particularly in elderly patients, as 25% to 50% of unexplained falls in this group may be related to syncope.30-32
The role of family history is controversial. Patients with a known family history of sudden cardiac death due to arrhythmogenic conditions such as long QT syndrome or Brugada syndrome may be at higher risk, especially if their ECG demonstrates a prolonged QTc (>460 ms) or spontaneous type 1 Brugada morphology.,33 Nonetheless, in the absence of an abnormal ECG, even patients with a positive family history may not be at increased risk.34 Note that cases of sudden cardiac death among younger people can be missed due to misclassification of a secondary event as the cause of death (drowning or motor vehicle crash).
The terms presyncope and near-syncope may be used to describe prodromal symptoms such as lightheadedness, sweating, nausea, or palpitations without a complete loss of consciousness. The outcomes of patients presenting with presyncope versus syncope do not appear to differ significantly, and the absence of a complete loss of consciousness should not alter the UC evaluation.35,36
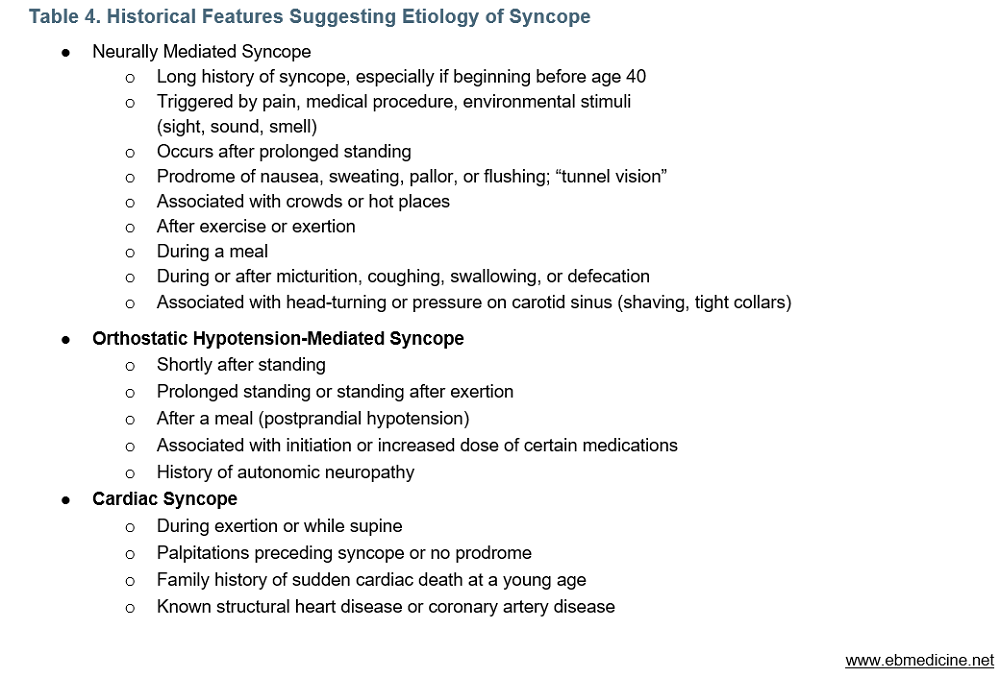
Inquire about known medical conditions, medications, herbal supplements, and other substances the patient is taking. Pay particular attention to any new or recently changed medications, as almost 40% of cases of orthostatic hypotension syncope may be drug induced.18 Patients with a history of cardiac disease, particularly heart failure, are at higher risk for adverse outcomes.37 See Table 4 for historical features that may indicate a particular category of syncope.
Role of Witnesses to Event
Witnesses to the event can be pivotal to the evaluation of patients with syncope by providing a description of the event as well as the minutes that followed. It is helpful to have witnesses recount the events preceding the loss of consciousness, its duration, any unusual movement during the event, and the patient’s orientation immediately following the event. Be aware that witnesses will often focus on any movement and label the episode as a “seizure;” asking witnesses to describe the exact movements observed will be helpful for the clinician in confirming the ultimate diagnosis.22 If a witness is not present in the UC but is available by telephone, it can be helpful to ask the patient to call the witness to assist with the history.
Physical Examination
In the postsyncopal patient, a targeted physical examination should be performed to detect findings that could indicate a life-threatening cause (tachycardia, bradycardia, hypotension, tachypnea, hypoxia, or neurologic deficits). In most patients who present with a sole complaint of syncope, the physical examination and vital signs will be normal. Look for evidence of hypovolemia or hypoperfusion, which may indicate hemorrhage or sepsis, and examine the abdomen to assess for tenderness or a pulsatile mass, which could indicate an abdominal aortic aneurysm. Bear in mind that young, thin patients can have palpable aortic pulses and not have an abdominal aortic aneurysm. Transient hypotension is expected with syncope, but persistent, unexplained low blood pressure indicates a more serious etiology. Consider obtaining orthostatic vital signs. Perform a careful neurologic examination to evaluate for subtle deficits that may indicate stroke.
Syncope is a frequent cause of significant injuries, with one study finding 6% of syncope patients experiencing fractures or motor vehicle crashes, and 29% incurring minor injuries such as lacerations and bruises.38 Particularly in older patients, a thorough physical examination should be performed to look for any evidence of trauma.
The cardiopulmonary examination is particularly important. Listen for irregular rhythms and murmurs and, if present, inquire as to any previous echocardiography or known diagnoses. Look for evidence of obstruction, such as distended neck veins or muffled heart sounds, and for evidence of heart failure, such as pulmonary rales and pedal edema.
Diagnostic Studies
Unless indicated by the history and physical examination, very few diagnostic studies aid in the evaluation of syncope. Imaging, in particular head computed tomography (CT), has a very low yield in determining the cause of syncope and should not be ordered unless it is independently indicated, eg, for associated focal neurological symptoms or signs or for imaging indicators relating to head trauma following syncope.
Electrocardiogram
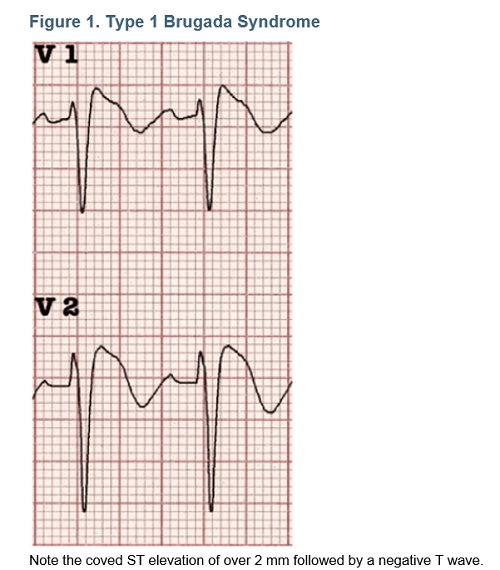
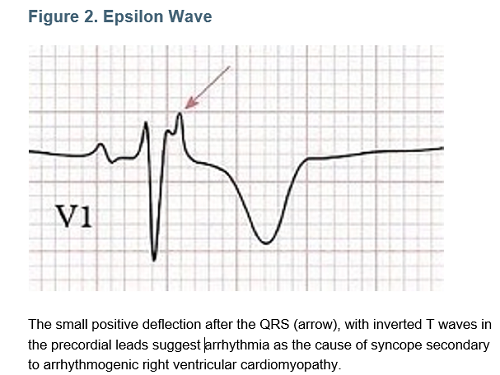
An ECG should be obtained for all patients with syncope. A reasonable exception is the patient who experiences a witnessed, obvious neurally mediated (vasovagal) syncope while in the UC center for another reason—for example, a 28-year-old needle-phobic patient who passes out while getting his local anesthetic injection. It’s crucial for UC clinicians to develop and maintain a high level of comfort with ECG interpretation in order to appropriately evaluate, counsel, and disposition syncopal patients. Review the ECG carefully to determine the underlying rhythm and rate, then look for conduction abnormalities such as pre-excitation or bundle branch block, ischemia and left ventricular hypertrophy, and rare findings such as type 1 Brugada morphology (see Figure 1) or epsilon waves associated with arrhythmogenic right ventricular cardiomyopathy (see Figure 2).
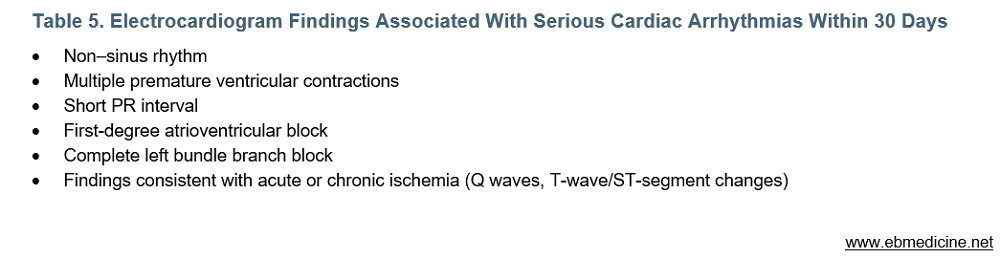
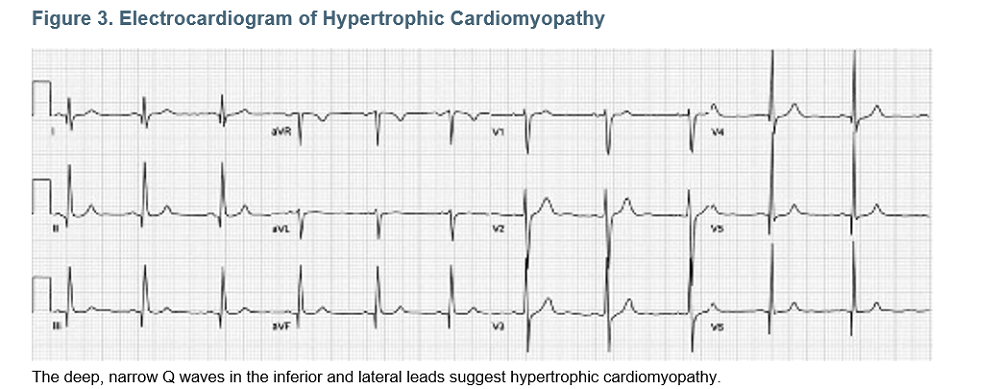
Some ECG findings are associated with serious cardiac arrhythmias within 30 days.39,40 (See Table 5.) A 2014 study found atrial fibrillation, intraventricular conduction disturbances, left ventricular hypertrophy, and ventricular pacing to be independent predictors of mortality.41 Other ECG findings that suggest a cardiac cause of syncope include Mobitz I atrioventricular block, inappropriate sinus bradycardia, early repolarization, and left ventricular hypertrophy, particularly if associated with “dagger” Q waves suggesting hypertrophic cardiomyopathy.6,42 (See Figure 3.)
Used with permission of Life in the Fastlane
Telemetry monitoring is not feasible in most UC settings, but it may be useful to observe/record continuous ECG monitoring for brief periods, especially in patients who are actively experiencing light-headedness or palpitations.
Laboratory Testing
Laboratory testing capabilities are often limited in the UC setting and laboratory studies are of low yield in patients with syncope unless the history or physical examination indicate a serious underlying disease process.43 For patients without a clear diagnosis of a low-risk syncope (such as vasovagal syncope), consider obtaining a glucose level, as well as a pregnancy test in women of child-bearing age. If suspicion exists that gastrointestinal bleeding is contributing to the presentation, perform fecal occult blood testing. If clinical features suggest significant anemia (eg, history of heavy menstrual periods, decreasing activity tolerance over time, conjunctival pallor), a point-of-care hemoglobin test can provide immediately useful data; however, in cases of rapid, acute blood loss, a single hemoglobin level can be falsely reassuring. Electrolyte panels and renal function tests are of limited value in patients not taking diuretics, patients without clinical features of significant dehydration, and patients who do not have a history or clinical presentation consistent with renal failure.
There is ongoing debate about the utility of cardiac biomarkers (troponin and B-type natriuretic peptide) in patients with otherwise undifferentiated syncope. These tests may have utility in patients with presentations that are worrisome for cardiac syncope (age >50 years, cardiac history, and/or risk factors), but are not necessary in otherwise low-risk patients and will not offer useful information in the UC setting. If there is serious concern for cardiac syncope, the patient is likely best served in the ED for telemetry and more thorough laboratory evaluation.
Pulmonary embolism is uncommon among patients presenting with syncope, and existing clinical decision rules (such as the pulmonary embolism rule-out criteria, or PERC) adequately identify patients with syncope and pulmonary embolism.44-47 Routine D-dimer measurement in patients with syncope without independent indications for evaluation of pulmonary embolism is not indicated.48,49
Imaging and Other Advanced Testing
Advanced imaging (particularly head CT) and chest x-rays are frequently obtained for syncope patients, despite their low yield.50 In the absence of neurological symptoms or indications for imaging in trauma by clinical decision rules, ED transfer for consideration of CT or magnetic resonance imaging is not indicated for patients with syncope.5,10,51
Treatment
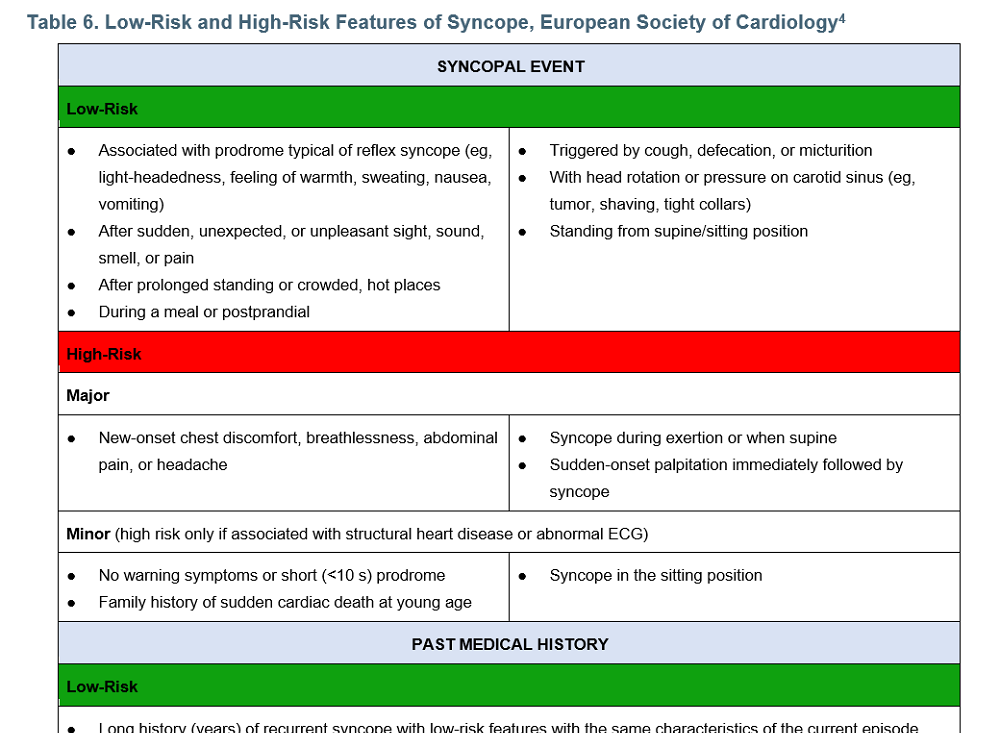
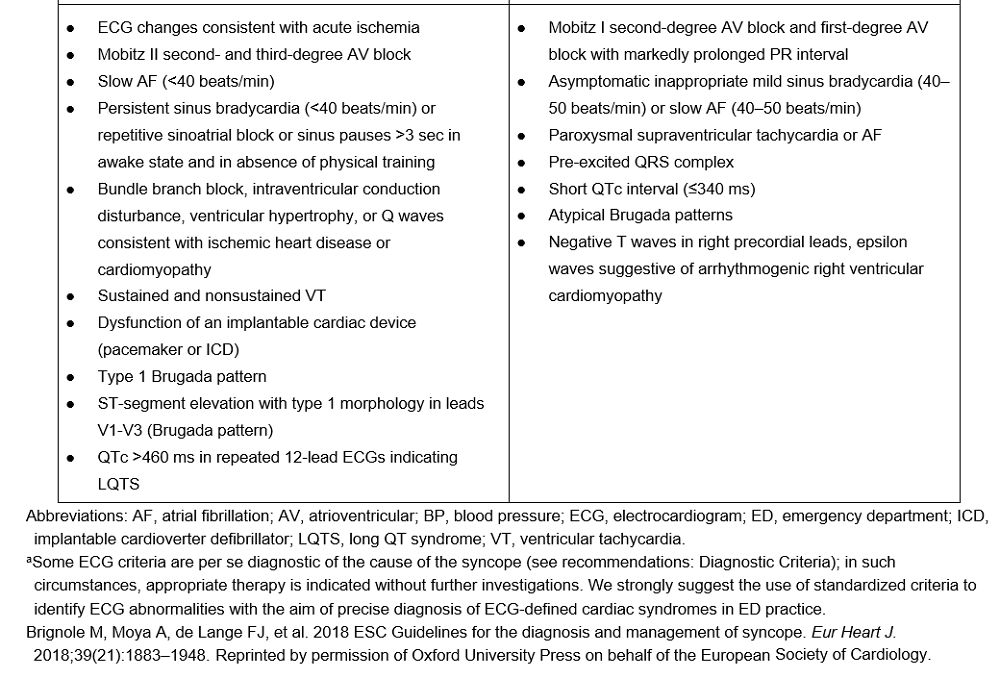
If no specific diagnosis is found after initial UC evaluation for syncope, the focus shifts to risk stratification of patients into high-risk or low-risk categories (see Table 6). The wide variety of definitions for adverse events and time frames makes consensus recommendations challenging. A 2010 study of more than 35,000 patients found a 3% chance of 7-day cardiac outcomes. Factors predictive for an adverse event included age >60 years, male gender, heart failure, coronary artery disease, abnormal ECG, or structural heart disease.52 A 2018 meta-analysis found that among patients with noncardiac or unexplained syncope, older, hypertensive, and diabetic patients had higher all-cause mortality.53

Clinical Risk-Stratification Tools
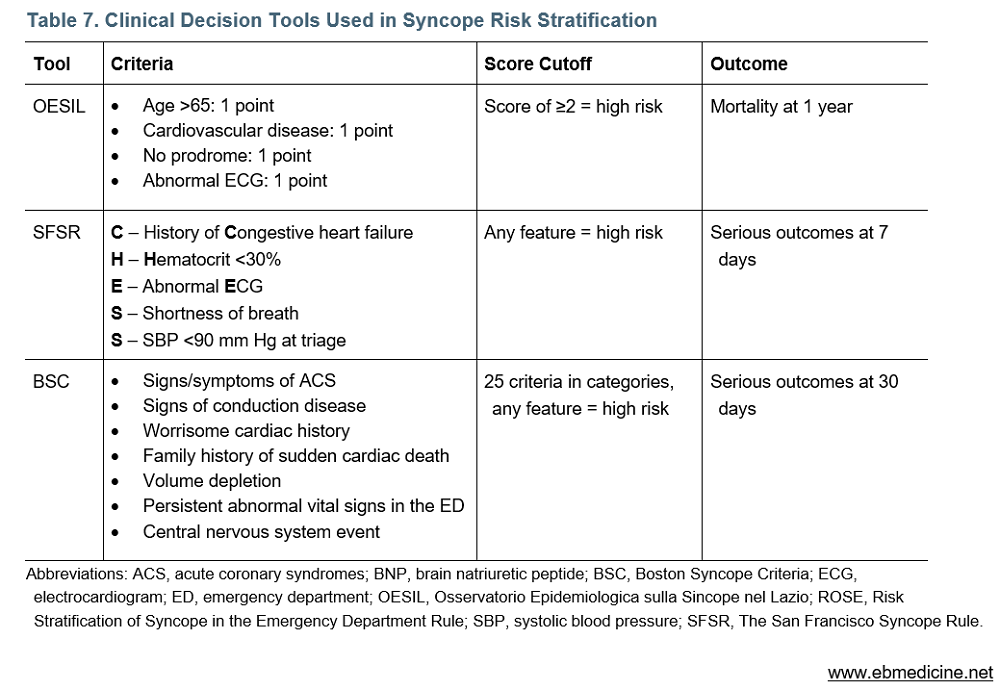
There are numerous risk stratification tools for syncopal patients, many of which have limited value in the UC setting. These risk-stratification tools should be applied only to patients for whom no apparent cause of syncope has been determined after the history, physical examination, and ECG interpretation. See Table 7, for a comparison of features of several risk-stratification tools, which are summarized following:
The OESIL (Osservatorio Epidemiologica sulla Sincope nel Lazio) risk score was derived in 2003 to predict 1-year mortality in patients presenting with syncope. Mortality increased from 9% for patients with 0 points to 57.1% for patients meeting all 4 criteria (4 points).54
The San Francisco Syncope Rule (SFSR) considers the presence of any of 5 features to indicate high risk. It was derived in 2004 to predict serious outcomes within 7 days and was reported to be 96% sensitive and 62% specific in derivation and 98% in prospective validation.55,56 Subsequent studies looked at 30-day outcomes. External validation studies found the sensitivity as low as 76%, and strict application of the rule may actually increase rather than decrease admissions.12,57,58
The Boston Syncope Criteria (BSC) consist of 25 features divided into 7 categories; any single feature is considered to indicate high risk. It was derived in 2007 and found to be 97% sensitive and 62% specific for adverse outcomes at 1 month.42 The lack of external validation and large number of criteria may limit its use in the ED or other settings.
Guidelines
2017 guidelines by the AHA/American College of Cardiology (ACC)59 and 2018 guidelines by the ESC4 support the use of a detailed history, physical examination, and ECG as the initial evaluation. In any setting, risk stratification rather than diagnosis should be performed in patients for whom the etiology remains uncertain. The use of clinical decision tools is considered reasonable, although outcomes in studies correlate strongly with the etiology assigned in the ED, and clinical decision tools should not replace physician judgment.25,60

Special Populations
Elderly Patients
The evaluation of syncope in older adults is particularly challenging, as many do not present with syncope, but rather with unexplained falls. Older adults are more likely to have underlying high-risk medical conditions, yet may still have benign causes of syncope. One-fourth of adults aged >50 years who present to the ED with a fall have symptoms suggestive of syncope or unexplained fall.31 There is no firm patient age that mandates an ED transfer or hospital admission following an episode of syncope, as the features of the event as well as other patient risk factors influence decision-making. However, it is reasonable to consider ED transfer for monitoring and cardiac biomarkers in patients >50 years who present with unexplained syncope. A 2016 study found almost half of older adults with dementia referred for unexplained falls received a diagnosis of syncope,32 and neurally mediated syncope is common in this age group.30 QTc prolongation may occur in 25% of elderly patients; increasing age or QTc >500 ms may predict 30-day and 1-year mortality.61,62
KidBits: The Syncopal Pediatric Patient
![]() The approach to syncope in children mirrors that of adults. The history, physical examination, and ECG are the most useful components of a syncope evaluation in children, and the vast majority of children have a benign etiology for syncope. One study found that neurally mediated syncope accounted for 80% of cases of children with syncope who underwent ED evaluation, and the majority of cases of cardiac syncope may be diagnosed by history, physical examination, and ECG.63 Family history, exertional syncope, syncope without prodrome, and syncope while supine may suggest a cardiac cause, and syncope associated with a loud noise (sudden adrenergic surge) should prompt evaluation for long QT syndrome.64 Pediatric patients with syncope often receive extensive evaluation, including head CT (58%, in one study) and laboratory testing, with very low yield, and 10% are admitted, with very few ultimately receiving a diagnosis of cardiac syncope.65
The approach to syncope in children mirrors that of adults. The history, physical examination, and ECG are the most useful components of a syncope evaluation in children, and the vast majority of children have a benign etiology for syncope. One study found that neurally mediated syncope accounted for 80% of cases of children with syncope who underwent ED evaluation, and the majority of cases of cardiac syncope may be diagnosed by history, physical examination, and ECG.63 Family history, exertional syncope, syncope without prodrome, and syncope while supine may suggest a cardiac cause, and syncope associated with a loud noise (sudden adrenergic surge) should prompt evaluation for long QT syndrome.64 Pediatric patients with syncope often receive extensive evaluation, including head CT (58%, in one study) and laboratory testing, with very low yield, and 10% are admitted, with very few ultimately receiving a diagnosis of cardiac syncope.65
Controversies
Orthostatic Vital Signs
Many guidelines recommend obtaining formal orthostatic vital signs on patients presenting with syncope. Although reasonable, there is likely some overlap between patients with asymptomatic changes in blood pressure and those with true orthostatic hypotension-mediated syncope. Note that the presence of orthostatic hypotension does not exclude more serious causes of syncope in the elderly.66,67 Identifying orthostasis may be beneficial to allow for modification of risk factors (such as medications) that may increase the likelihood of falls, but it should not be used as the sole factor in risk stratification.
Disposition
High-Risk Patients
Patients with an identified life-threatening diagnosis should receive immediate stabilization and prompt ED transfer; they need not undergo syncope risk stratification. Patients with syncope that remains unexplained after the history, physical examination, ECG, and initial testing should be risk stratified using appropriate clinical features, and those with any high-risk features should be considered for ED transfer.
Intermediate-Risk Patients
For patients without high-risk or low-risk features, ED transfer should be considered so that a more exhaustive workup and longer monitoring period can be undertaken. Intermediate-risk factors include age ≥50 years, prior history of cardiac disease, cardiac device without evidence of dysfunction or concerning ECG findings, family history of sudden cardiac death, and symptoms not consistent with reflex-mediated syncope.59 Engage in shared decision-making regarding ED transfer versus outpatient follow-up, and ensure close follow-up for patients who decide against ED transfer as many patients in this category may benefit from further testing, including tilt-table testing, implantable loop recorder, electrophysiology evaluation, or other continuous ambulatory electrocardiographic monitoring.68
Low-Risk Patients
Low-risk patients, even those with unexplained syncope, should generally be discharged. Follow-up may be appropriate for patients with recurrent syncope or those without clearly benign causes. Even among patients with low-risk syncope, approximately 9% may have recurrence within 6 months, with 3 or more lifetime incidents most predictive of future recurrence.69 Be familiar with state laws regarding release for driving and consider referral before return to work for commercial drivers or others with a high risk for injury if syncope recurs.70
Summary
Syncope is a common, usually benign presentation resulting from transient cerebral hypoperfusion. It does not require extensive investigation or ED transfer unless there are indications for a life-threatening process or certain high-risk features. An appropriate, focused history, physical examination, and ECG are the most important tools in identifying the cause of syncope or identifying low-risk patients who may be discharged from urgent care. For patients in whom the cause is unclear after a careful history, physical examination, and ECG have been performed, targeted laboratory testing may be helpful. ED transfer for investigations not otherwise indicated by the history and physical examination, especially advanced neuroimaging, have very low yield and should generally be avoided.
Society guidelines and multiple clinical decision tools have attempted, with some success, to help identify the subset of patients with syncope who are at high risk for mortality and other adverse outcomes. Certain features commonly included in risk-stratification scores, such as cardiac disease (especially heart failure) and abnormal ECG, may be associated with increased risk for short-term mortality and other adverse events.
Time and Cost-Effective Strategies
- Obtain an ECG on all syncope patients (except those with in-clinic, witnessed, clearly neurally mediated vasovagal syncope), and a pregnancy test in all women of child-bearing age. Otherwise, limit testing and imaging in patients for whom there is no concern for immediately life-threatening conditions such as myocardial infarction, aortic dissection, pulmonary embolism, etc.
- Review ECGs carefully for the presence of high-risk features such as non-sinus rhythm, ectopy, conduction abnormalities including atrioventricular block and left bundle branch block, acute or chronic ischemia, abnormal intervals, and inherited conditions including hypertrophic cardiomyopathy and Brugada or long QT syndromes.
- Do not order a head CT or transfer syncopal patients to the ED for consideration of neuroimaging in the absence of positive neurologic findings or suspicion for subarachnoid hemorrhage.
- Obtain orthostatic vital signs in syncope patients to identify modifiable causes of orthostatic hypotension, but be cautious of incidental orthostasis in high-risk patients, especially the elderly.
- Avoid transfer low-risk patients to the ED unless injuries or other indications exist.
- Use clinical judgment, patient preference, and scientific evidence to inform disposition decisions. Currently, there is no uniformly-accepted risk stratification tool for syncopal patients.
Risk Management Pitfalls For Management of Syncope in Urgent Care
![]() “It sounded like vasovagal syncope, so I didn’t get an ECG.” Although ECGs in patients with suspected vasovagal syncope may often be normal, it is a level 1 recommendation by both the AHA and ESC to obtain an ECG in all patients with syncope. This inexpensive, noninvasive test may reveal underlying pathology that can change management dramatically.
“It sounded like vasovagal syncope, so I didn’t get an ECG.” Although ECGs in patients with suspected vasovagal syncope may often be normal, it is a level 1 recommendation by both the AHA and ESC to obtain an ECG in all patients with syncope. This inexpensive, noninvasive test may reveal underlying pathology that can change management dramatically.
“A witness reported a seizure, so I didn’t work up the patient for syncope.” Witnesses often interpret any convulsive activity as a seizure. Consider features such as tongue laceration or prolonged postictal period to diagnose syncope accurately and avoid unnecessary evaluation or restrictions on activity after discharge.
“The 88-year-old patient had orthostasis, so I didn’t think he needed an ED transfer for syncope. I told him to aggressively hydrate at home and follow up with his PCP next week.” The presence of orthostasis does not reliably exclude more serious causes of syncope, particularly in elderly patients. Orthostatic vital signs must be interpreted in the context of the history, physical examination, and other risk factors to avoid missing serious disease.
“The patient didn’t mention chest pain, so I didn’t consider pulmonary embolism.” Pulmonary embolism is an uncommon cause of syncope but should be considered in patients with unexplained, persistently abnormal vital signs, especially hypotension, tachypnea, or tachycardia.
“The hemoglobin was normal, so I ruled out a gastrointestinal bleed as the cause.” Acute blood loss may not be reflected in an initial hemoglobin result. Consider fecal occult blood testing in patients for whom the history or examination are suspicious for gastrointestinal bleeding.
“The ECG showed only sinus tachycardia, so I didn’t do any further testing.” Abnormal vital signs that persist do not support a benign cause of syncope, and an appropriate evaluation and/or ED transfer guided by the history and physical examination should be performed.
“I thought her abdominal pain was from her vagal episode, so I didn’t order a pregnancy test.” Nausea and abdominal pain may accompany vasovagal syncope and persist following the episode, but any patient with syncope and abdominal pain should undergo appropriate testing to exclude more serious conditions.
“Since his ED evaluation was unremarkable and he had no high-risk features, I released the 31-year-old high-rise construction worker to go back to work.” Syncope recurrence is common, but sometimes challenging to predict. Many patients with neurally-mediated syncope may be safely released to return to driving, but certain high-risk occupations may require referral before returning to employment.
Critical Appraisal of the Literature
A literature search from January 1970 to December 2020 was performed in PubMed, Embase®, the Cochrane Database of Systematic Reviews, and the Cochrane Central Register of Controlled Trials, using MeSH terms including syncope, death, hospitalization, risk assessment, and emergency. The intent of the literature search was to identify studies relevant to the epidemiology, ED evaluation, and risk stratification of patients presenting with syncope. A total of 1288 abstracts were screened, and 380 full-text studies reviewed for inclusion, with 117 studies included. Practice guidelines from professional societies including the American College of Emergency Physicians (ACEP), the European Society of Cardiology (ESC), and the American Heart Association (AHA) were reviewed.
Although there are numerous studies examining syncope, many are database reviews or retrospective reviews. The definitions used for syncope and its categorizations vary considerably and, between studies, the populations are often quite heterogeneous. Risk-stratification tools often perform poorly in subsequent validation studies.71-73 Most prospective studies have small sample sizes, which is problematic, as the low rate of serious adverse events makes it challenging to detect significant relationships reliably. Overall, the syncope literature consists primarily of observational studies and database studies, which are assigned a low quality of evidence. The plethora of clinical decision rules underscore the challenge associated with distilling such a varied presentation and population into a concise set of recommendations.
Case Conclusions
VS and ECG were normal, and the patient had no complaints in clinic. The description of the event strongly suggested neurally mediated (vasovagal) syncope, and you reassured her parents that a head CT was not indicated since there was no head trauma and she had a normal neurologic exam. She was eager to go home, and the parents were grateful to have avoided ED transfer and possible unnecessary radiation exposure.
You noted that the man had no tongue trauma, and there was no reported postictal period, so your concern for seizure was very low. However, the tachycardia, hypoxia, and tachypnea with borderline systolic blood pressure after his surgery 3 weeks earlier raised your concern for pulmonary embolism. You placed him on supplemental oxygen, obtained an ECG, and activated EMS. The ECG showed sinus tachycardia and an incomplete right bundle branch block. Submassive pulmonary embolism was diagnosed via chest CT in the ED, and the patient was admitted to the ICU for thrombolytic therapy.
The woman’s unexplained fall and comorbidities led you to obtain an ECG, which showed a QTc of 500 ms. You activated EMS, and while in the ED, she had an episode of nonsustained ventricular tachycardia. She was admitted to a monitored bed for continuous telemetry and cardiology consultation, and she received an implantable cardioverter/defibrillator prior to discharge.
Charting Tips
![]() Syncope can be the result of causes ranging from benign to life threatening. A detailed history and physical examination, along with an ECG, are among the most important aspects of the workup for a postsyncopal patient, and must be documented.
Syncope can be the result of causes ranging from benign to life threatening. A detailed history and physical examination, along with an ECG, are among the most important aspects of the workup for a postsyncopal patient, and must be documented.
History
- Activity before and after the event, exertional activity, prodromal symptoms
- Duration of event and time to return to baseline
- Past medical history of coronary artery disease, pacemaker, defibrillator, or dysrhythmia
- Previous episodes
- Previous workup
- Input from bystander/family
Physical Examination
- Address any abnormal vital signs, especially persistent bradycardia and tachycardia
- New or undiagnosed murmur
- Abdominal tenderness, rectal exam, color of conjunctiva
Electrocardiogram
- Look for ischemic changes
- Mobitz II second- and third-degree atrioventricular block
- Intraventricular conduction delays
- Compare to previous ECGs if possible
— Patrick O’Malley, MD
Clinical Pathway for Urgent Care Evaluation of Patients Presenting With Transient Loss of Consciousness
Tables and Figures
Used with permission of Life in the Fastlane
References
Evidence-based medicine requires a critical appraisal of the literature based upon study methodology and number of subjects. Not all references are equally robust. The findings of a large, prospective, randomized, and blinded trial should carry more weight than a case report.
To help the reader judge the strength of each reference, pertinent information about the study, such as the type of study and the number of patients in the study is included in bold type following the references, where available. The most informative references cited in this paper, as determined by the author, are noted by an asterisk (*) next to the number of the reference.
- Sun BC, Emond JA, Camargo CA, Jr. Characteristics and admission patterns of patients presenting with syncope to U.S. emergency departments, 1992-2000. Acad Emerg Med. 2004;11(10):1029-1034. (Database analysis)
- Kadri AN, Abuamsha H, Nusairat L, et al. Causes and predictors of 30-day readmission in patients with syncope/collapse: a nationwide cohort study. J Am Heart Assoc. 2018;7(18):e009746. (Database analysis)
- Joy PS, Kumar G, Olshansky B. Syncope: outcomes and conditions associated with hospitalization. Am J Med. 2017;130(6):699-706.e696. (Database analysis)
- * Brignole M, Moya A, de Lange FJ, et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur Heart J. 2018;39(21):1883-1948. (Guidelines)
- Ozturk K, Soylu E, Bilgin C, et al. Predictor variables of abnormal imaging findings of syncope in the emergency department. Int J Emerg Med. 2018;11(1):16. (Retrospective; 1230 patients)
- Gatzoulis KA, Karystinos G, Gialernios T, et al. Correlation of noninvasive electrocardiography with invasive electrophysiology in syncope of unknown origin: implications from a large syncope database. Ann Noninvasive Electrocardiol. 2009;14(2):119-127. (Retrospective; 421 patients)
- Chiu DT, Shapiro NI, Sun BC, et al. Are echocardiography, telemetry, ambulatory electrocardiography monitoring, and cardiac enzymes in emergency department patients presenting with syncope useful tests? A preliminary investigation. J Emerg Med. 2014;47(1):113-118. (Prospective observational; 570 patients)
- Anderson KL, Limkakeng A, Damuth E, et al. Cardiac evaluation for structural abnormalities may not be required in patients presenting with syncope and a normal ECG result in an observation unit setting. Ann Emerg Med. 2012;60(4):478-484.e471. (Retrospective; 323 patients)
- AlJaroudi WA, Alraies MC, Wazni O, et al. Yield and diagnostic value of stress myocardial perfusion imaging in patients without known coronary artery disease presenting with syncope. Circ Cardiovasc Imaging. 2013;6(3):384-391. (Retrospective; 700 patients)
- Viau JA, Chaudry H, Hannigan A, et al. The yield of computed tomography of the head among patients presenting with syncope: a systematic review. Acad Emerg Med. 2019;26(5):479-490. (Meta-analysis; 3361 patients)
- Deif B, Kang S, Ismail A, et al. Application of syncope guidelines in the emergency department do not reduce admission rates: a retrospective cohort study. Can J Cardiol. 2018;34(9):1158-1164. (Retrospective; 1031 patients)
- Sun BC, Mangione CM, Merchant G, et al. External validation of the San Francisco Syncope Rule. Ann Emerg Med. 2007;49(4):420-427, 427.e421-424. (Prospective observational; 477 patients)
- Soteriades ES, Evans JC, Larson MG, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878-885. (Retrospective; 727 patients)
- Derose SF, Gabayan GZ, Chiu VY, et al. Patterns and preexisting risk factors of 30-day mortality after a primary discharge diagnosis of syncope or near syncope. Acad Emerg Med. 2012;19(5):488-496. (Retrospective; 22,189 patients)
- * D’Ascenzo F, Biondi-Zoccai G, Reed MJ, et al. Incidence, etiology and predictors of adverse outcomes in 43,315 patients presenting to the Emergency Department with syncope: an international meta-analysis. Int J Cardiol. 2013;167(1):57-62. (Meta-analysis; 43,315 patients)
- Del Rosso A, Alboni P, Brignole M, et al. Relation of clinical presentation of syncope to the age of patients. Am J Cardiol. 2005;96(10):1431-1435. (Prospective; 485 patients)
- Shiyovich A, Munchak I, Zelingher J, et al. Admission for syncope: evaluation, cost and prognosis according to etiology. Isr Med Assoc J. 2008;10(2):104-108. (Retrospective; 376 patients)
- Sarasin FP, Louis-Simonet M, Carballo D, et al. Prevalence of orthostatic hypotension among patients presenting with syncope in the ED. Am J Emerg Med. 2002;20(6):497-501. (Prospective observational; 650 patients)
- White JL, Hollander JE, Chang AM, et al. Orthostatic vital signs do not predict 30 day serious outcomes in older emergency department patients with syncope: a multicenter observational study. Am J Emerg Med. 2019;37(12):2215-2223. (Prospective observational; 1974 patients)
- Ruwald MH, Ruwald AC, Jons C, et al. Evaluation of the CHADS2 risk score on short- and long-term all-cause and cardiovascular mortality after syncope. Clin Cardiol. 2013;36(5):262-268. (Database analysis)
- Hoefnagels WA, Padberg GW, Overweg J, et al. Transient loss of consciousness: the value of the history for distinguishing seizure from syncope. J Neurol. 1991;238(1):39-43. (Prospective observational; 94 patients)
- Shmuely S, Bauer PR, van Zwet EW, et al. Differentiating motor phenomena in tilt-induced syncope and convulsive seizures. Neurology. 2018;90(15):e1339-e1346. (Prospective observational; 115 patients)
- Sheldon R, Rose S, Ritchie D, et al. Historical criteria that distinguish syncope from seizures. J Am Coll Cardiol. 2002;40(1):142-148. (Prospective observational; 539 patients)
- Brigo F, Nardone R, Ausserer H, et al. The diagnostic value of urinary incontinence in the differential diagnosis of seizures. Seizure. 2013;22(2):85-90. (Meta-analysis; 473 patients)
- Toarta C, Mukarram M, Arcot K, et al. Syncope prognosis based on emergency department diagnosis: a prospective cohort study. Acad Emerg Med. 2018;25(4):388-396. (Prospective observational; 5010 patients)
- Sud S, Klein GJ, Skanes AC, et al. Predicting the cause of syncope from clinical history in patients undergoing prolonged monitoring. Heart Rhythm. 2009;6(2):238-243. (Prospective; 119 patients)
- Chang AM, Hollander JE, Su E, et al. Recurrent syncope is not an independent risk predictor for future syncopal events or adverse outcomes. Am J Emerg Med. 2019;37(5):869-872. (Prospective observational; 3580 patients)
- Solbiati M, Casazza G, Dipaola F, et al. Syncope recurrence and mortality: a systematic review. Europace. 2015;17(2):300-308. (Meta-analysis; 11,158 patients)
- Aydin MA, Maas R, Mortensen K, et al. Predicting recurrence of vasovagal syncope: a simple risk score for the clinical routine. J Cardiovasc Electrophysiol. 2009;20(4):416-421. (Prospective observational; 276 patients)
- Anpalahan M, Gibson S. The prevalence of neurally mediated syncope in older patients presenting with unexplained falls. Eur J Intern Med. 2012;23(2):e48-52. (Prospective; 200 patients)
- Bhangu J, Hall P, Devaney N, et al. The prevalence of unexplained falls and syncope in older adults presenting to an Irish urban emergency department. Eur J Emerg Med. 2019;26(2):100-104. (Prospective observational; 561 patients)
- Ungar A, Mussi C, Ceccofiglio A, et al. Etiology of syncope and unexplained falls in elderly adults with dementia: Syncope and Dementia (SYD) Study. J Am Geriatr Soc. 2016;64(8):1567-1573. (Prospective observational; 357 patients)
- Okamura H, Kamakura T, Morita H, et al. Risk stratification in patients with Brugada syndrome without previous cardiac arrest – prognostic value of combined risk factors. Circ J. 2015;79(2):310-317. (Retrospective; 218 patients)
- Sarkozy A, Sorgente A, Boussy T, et al. The value of a family history of sudden death in patients with diagnostic type I Brugada ECG pattern. Eur Heart J. 2011;32(17):2153-2160. (Prospective observational; 280 patients)
- Thiruganasambandamoorthy V, Stiell IG, Wells GA, et al. Outcomes in presyncope patients: a prospective cohort study. Ann Emerg Med. 2015;65(3):268-276.e266. (Prospective observational; 881 patients)
- Roncon L, Zuin M, Casazza F, et al. Impact of syncope and pre-syncope on short-term mortality in patients with acute pulmonary embolism. Eur J Intern Med. 2018;54:27-33. (Prospective; 1716 patients)
- Aro AL, Rusinaru C, Uy-Evanado A, et al. Syncope and risk of sudden cardiac arrest in coronary artery disease. Int J Cardiol. 2017;231:26-30. (Case control; 2119 patients)
- Kapoor WN, Peterson J, Wieand HS, et al. Diagnostic and prognostic implications of recurrences in patients with syncope. Am J Med. 1987;83(4):700-708. (Prospective observational; 433 patients)
- Sun BC, Hoffman JR, Mower WR, et al. Low diagnostic yield of electrocardiogram testing in younger patients with syncope. Ann Emerg Med. 2008;51(3):240-246, 246.e241. (Prospective observational; 477 patients)
- Nishijima DK, Lin AL, Weiss RE, et al. ECG predictors of cardiac arrhythmias in older adults with syncope. Ann Emerg Med. 2018;71(4):452-461.e453. (Prospective observational; 3416 patients)
- Pérez-Rodon J, Martínez-Alday J, Barón-Esquivias G, et al. Prognostic value of the electrocardiogram in patients with syncope: data from the group for syncope study in the emergency room (GESINUR). Heart Rhythm. 2014;11(11):2035-2044. (Retrospective observational; 524 patients)
- Grossman SA, Fischer C, Lipsitz LA, et al. Predicting adverse outcomes in syncope. J Emerg Med. 2007;33(3):233-239. (Prospective observational; 362 patients)
- DeLorenzo R. Syncope. In: Marx J, Hockberger R, Walls R, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 5th ed: Mosby; 2002. (Textbook chapter)
- Thiruganasambandamoorthy V, Sivilotti MLA, Rowe BH, et al. Prevalence of pulmonary embolism among emergency department patients with syncope: a multicenter prospective cohort study. Ann Emerg Med. 2019;73(5):500-510. (Prospective observational; 9091 patients)
- Costantino G, Ruwald MH, Quinn J, et al. Prevalence of pulmonary embolism in patients with syncope. JAMA Intern Med. 2018;178(3):356-362. (Database analysis)
- Oqab Z, Ganshorn H, Sheldon R. Prevalence of pulmonary embolism in patients presenting with syncope. A systematic review and meta-analysis. Am J Emerg Med. 2018;36(4):551-555. (Meta-analysis; 7583 patients)
- Raynal PA, Cachanado M, Truchot J, et al. Prevalence of pulmonary embolism in emergency department patients with isolated syncope: a prospective cohort study. Eur J Emerg Med. 2019;26(6):458-461. (Prospective; 411 patients)
- Stockley CJ, Reed MJ, Newby DE, et al. The utility of routine D-dimer measurement in syncope. Eur J Emerg Med. 2009;16(5):256-260. (Prospective; 237 patients)
- Kelly C, Bledsoe JR, Woller SC, et al. Diagnostic yield of pulmonary embolism testing in patients presenting to the emergency department with syncope. Res Pract Thromb Haemost. 2020;4(2):263-268. (Retrospective; 32,440 patients)
- Chou SC, Nagurney JM, Weiner SG, et al. Trends in advanced imaging and hospitalization for emergency department syncope care before and after ACEP clinical policy. Am J Emerg Med. 2019;37(6):1037-1043. (Database analysis)
- İdil H, Kılıc TY. Diagnostic yield of neuroimaging in syncope patients without high-risk symptoms indicating neurological syncope. Am J Emerg Med. 2019;37(2):228-230. (Retrospective; 1114 patients)
- Gabayan GZ, Derose SF, Asch SM, et al. Predictors of short-term (seven-day) cardiac outcomes after emergency department visit for syncope. Am J Cardiol. 2010;105(1):82-86. (Database analysis; 35,340 patients)
- Ricci F, Sutton R, Palermi S, et al. Prognostic significance of noncardiac syncope in the general population: a systematic review and meta-analysis. J Cardiovasc Electrophysiol. 2018;29(12):1641-1647. (Meta-analysis; 38,843 patients)
- Colivicchi F, Ammirati F, Melina D, et al. Development and prospective validation of a risk stratification system for patients with syncope in the emergency department: the OESIL risk score. Eur Heart J. 2003;24(9):811-819. (Prospective; 270 patients derivation, 328 validation)
- Quinn JV, Stiell IG, McDermott DA, et al. Derivation of the San Francisco Syncope Rule to predict patients with short-term serious outcomes. Ann Emerg Med. 2004;43(2):224-232. (Prospective; 684 patients)
- Quinn J, McDermott D, Stiell I, et al. Prospective validation of the San Francisco Syncope Rule to predict patients with serious outcomes. Ann Emerg Med. 2006;47(5):448-454. (Prospective; 791 patients)
- Saccilotto RT, Nickel CH, Bucher HC, et al. San Francisco Syncope Rule to predict short-term serious outcomes: a systematic review. Cmaj. 2011;183(15):E1116-1126. (Meta-analysis; 5316 patients)
- Birnbaum A, Esses D, Bijur P, et al. Failure to validate the San Francisco Syncope Rule in an independent emergency department population. Ann Emerg Med. 2008;52(2):151-159. (Prospective observational; 743 patients)
- * Shen WK, Sheldon RS, Benditt DG, et al. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2017;70(5):e39-e110. (Guidelines)
- Albassam OT, Redelmeier RJ, Shadowitz S, et al. Did this patient have cardiac syncope?: The Rational Clinical Examination Systematic Review. Jama. 2019;321(24):2448-2457. (Meta-analysis; 4317 patients)
- White JL, Chang AM, Hollander JE, et al. QTc prolongation as a marker of 30-day serious outcomes in older patients with syncope presenting to the emergency department. Am J Emerg Med. 2019;37(4):685-689. (Prospective observational; 2609 patients)
- Bo M, Ceccofiglio A, Mussi C, et al. Prevalence, predictors and clinical implications of prolonged corrected QT in elderly patients with dementia and suspected syncope. Eur J Intern Med. 2019;61:34-39. (Prospective observational; 432 patients)
- Massin MM, Bourguignont A, Coremans C, et al. Syncope in pediatric patients presenting to an emergency department. J Pediatr. 2004;145(2):223-228. (Prospective observational; 226 patients)
- Sanatani S, Chau V, Fournier A, et al. Canadian Cardiovascular Society and Canadian Pediatric Cardiology Association position statement on the approach to syncope in the pediatric patient. Can J Cardiol. 2017;33(2):189-198. (Review article)
- Goble MM, Benitez C, Baumgardner M, et al. ED management of pediatric syncope: searching for a rationale. Am J Emerg Med. 2008;26(1):66-70. (Retrospective; 140 patients)
- Mussi C, Ungar A, Salvioli G, et al. Orthostatic hypotension as cause of syncope in patients older than 65 years admitted to emergency departments for transient loss of consciousness. J Gerontol A Biol Sci Med Sci. 2009;64(7):801-806. (Prospective; 259 patients)
- Schaffer JT, Keim SM, Hunter BR, et al. Do orthostatic vital signs have utility in the evaluation of syncope? J Emerg Med. 2018;55(6):780-787. (Review article)
- Probst MA, Lin MP, Sze JJ, et al. Shared decision making for syncope in the emergency department: a randomized controlled feasibility trial. Acad Emerg Med. 2020;27(9):853-865. (Randomized controlled trial; 50 patients)
- Barbic F, Dipaola F, Casazza G, et al. Syncope in a working-age population: recurrence risk and related risk factors. J Clin Med. 2019;8(2). (Prospective observational; 348 patients)
- Sorajja D, Nesbitt GC, Hodge DO, et al. Syncope while driving: clinical characteristics, causes, and prognosis. Circulation. 2009;120(11):928-934. (Case-control; 381 patients)
- Thiruganasambandamoorthy V, Hess EP, Alreesi A, et al. External validation of the San Francisco Syncope Rule in the Canadian setting. Ann Emerg Med. 2010;55(5):464-472. (Retrospective; 490 patients)
- Serrano LA, Hess EP, Bellolio MF, et al. Accuracy and quality of clinical decision rules for syncope in the emergency department: a systematic review and meta-analysis. Ann Emerg Med. 2010;56(4):362-373.e361. (Meta-analysis; 10,994 patients)
- Barón-Esquivias G, Fernández-Cisnal A, Arce-León Á, et al. Prognosis of patients with syncope seen in the emergency room department: an evaluation of four different risk scores recommended by the European Society of Cardiology guidelines. Eur J Emerg Med. 2017;24(6):428-434. (Prospective observational; 323 patients)







