

|
|
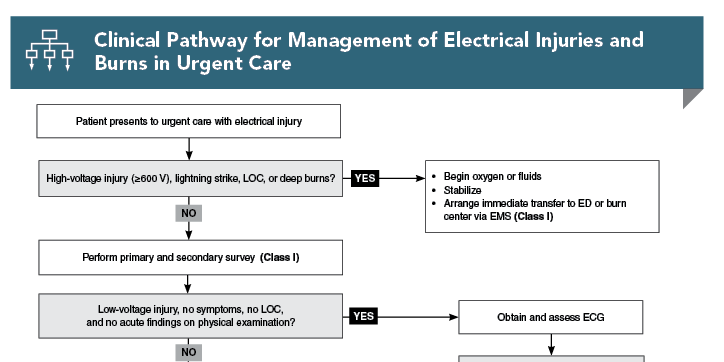
Electrical injuries cause approximately 1000 deaths per year in the United States, most often due to either high-voltage electrical injury or lightning strike. However, an additional approximately 30,000 nonfatal shocks occur annually. The type of exposure will guide the management strategy for patients with electrical injury. While most patients with low-risk injuries can be safely managed in and discharged from urgent care, clinicians must be able to recognize high-risk injuries that require transfer to a higher level of care. This review provides evidence-based recommendations for the evaluation and management of electrical injuries in the urgent care setting, including indications for referral to an emergency department or comprehensive burn center.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
2. * Rabban JT, Blair JA, Rosen CL, et al. Mechanisms of pediatric electrical injury. New implications for product safety and injury prevention. Arch Pediatr Adolesc Med. 1997;151(7):696-700. (Case series; 144 pediatric and adolescent patients) DOI: 10.1001/archpedi.1997.02170440058010
3. * Gurbuz K, Demir M. Patterns and outcomes of high-voltage vs low-voltage pediatric electrical injuries: an 8-year retrospective analysis of a tertiary-level burn center. J Burn Care Res. 2022;43(3):704-709. (Retrospective analysis; 2243 patients) DOI: 10.1093/jbcr/irab178
9. * O’Keefe Gatewood M, Zane RD. Lightning injuries. Emerg Med Clin North Am. 2004;22(2):369-403. (Review) DOI: 10.1016/j.emc.2004.02.002
10. * Spies C, Trohman RG. Narrative review: electrocution and life-threatening electrical injuries. Ann Intern Med. 2006;145(7):531-537. (Narrative review) DOI: 10.7326/0003-4819-145-7-200610030-00011
19. * Davis C, Engeln A, Johnson EL, et al. Wilderness Medical Society practice guidelines for the prevention and treatment of lightning injuries: 2014 update. Wilderness Environ Med. 2014;25(4 Suppl):S86-S95. (Practice guidelines) DOI: 10.1016/j.wem.2014.08.011
27. * O’Keefe KP. Electrical injuries and lightning strikes: evaluation and management. In: Danzel DF, Moreira ME, eds. UpToDate. Wolters Kluwer; 2024. (Online textbook chapter)
28. * American Burn Association. Guidelines for Burn Patient Referral. Accessed March 10, 2024. (Practice guidelines)
32. * Haileyesus T, Annest JL, Mercy JA. Non-fatal conductive energy device-related injuries treated in US emergency departments, 2005-2008. Inj Prev. 2011;17(2):127-130. (Retrospective study; 75,000 patients per year) DOI: 10.1136/ip.2010.028704
34. * Kroll MW, Lakkireddy DR, Stone JR, et al. TASER electronic control devices and cardiac arrests: coincidental or causal? Circulation. 2014;129(1):93-100. (Response article) DOI: 10.1161/CIRCULATIONAHA.113.004401
Subscribe to get the full list of 39 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: electrical, low voltage, high voltage, current, shock, burn, oral commissure, lightning strike, arrhythmia, compartment syndrome, TASER, myoglobinuria, Rule of 9s, Lund Browder, Parkland formula, modified Brooke formula
Nathan J. Morrison, DO, MEng; Robert Olympia, MD
Margaret J. Carman, DNP, RN, ACNP-BC, ENP-BC, CHSE, FAEN; Joseph Toscano, MD, FCUCM
April 1, 2024
April 1, 2027 CME Information
4 AMA PRA Category 1 Credits™. 4 AOA Category 2-B Credits. 4 AAFP Prescribed Credits Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 4 Trauma CME credit.
Evidence-Based Urgent Care • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Evidence-Based Urgent Care issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933