

|
|
Pediatric ingestions present a common challenge for emergency clinicians. While findings and information from the physical examination, electrocardiographic, laboratory, and radiologic testing may suggest a specific ingestion, timely identification of many substances is not always possible. In addition to diagnostic challenges, the management of many ingested substances is controversial and recommendations are evolving. This issue reviews the initial resuscitation, diagnosis, and treatment of common pediatric ingestions. Also discussed are current recommendations for decontamination and administration of antidotes for specific toxins.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
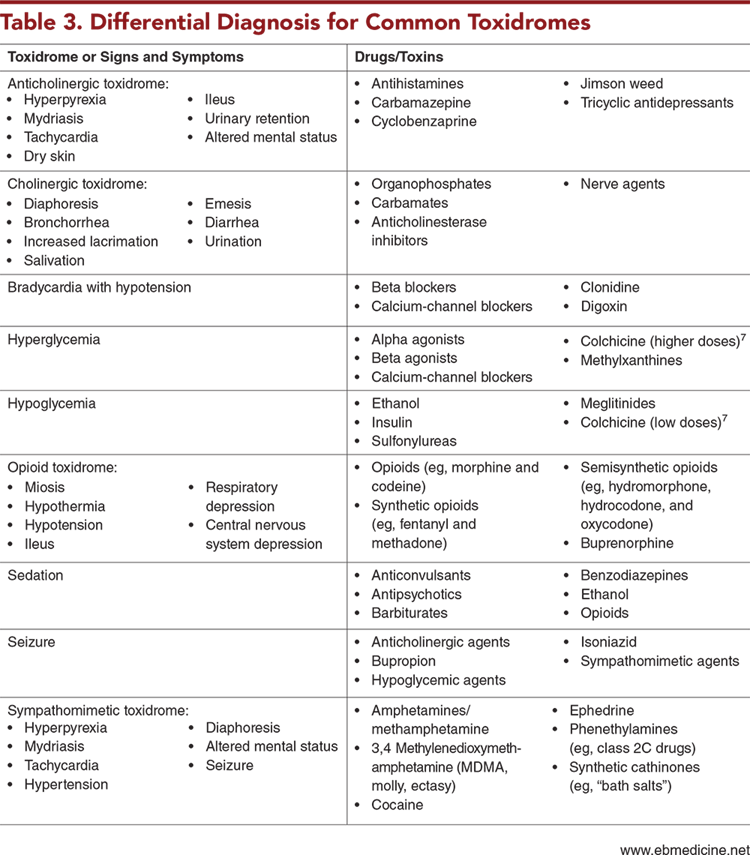
3. “The parents didn’t mention giving aspirin to their febrile child, so I didn’t consider it.” Symptoms of a toxic ingestion may be nonspecific, and an elevated temperature may be due to ingestion of salicylates, anticholinergic agents, or sympathomimetic agents, in addition to an infectious process. Always ask about use of over-the-counter medications and their ingredients.
4. “The urine toxicology screen was negative, so ingestion was ruled out.” Urine toxicology screen interpretations are limited by which drugs are included and at what threshold levels, in addition to false-negative and false-positive results.
7. “We gave dextrose to prevent hypoglycemia after suspected sulfonylurea ingestion.” Prophylactic dextrose will mask and possibly delay effects of sulfonylurea ingestion, confusing further management. Dextrose should be administered only as needed.
Subscribe to access the complete Risk Management Pitfalls to guide your clinical decision making.
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
4. * Bar-Oz B, Levichek Z, Koren G. Medications that can be fatal for a toddler with one tablet or teaspoonful: a 2004 update. Paediatr Drugs. 2004;6(2):123-126. (Review) DOI: 10.2165/00148581-200406020-00005
5. US Consumer Product Safety Commission. Poison prevention packaging - a guide for healthcare professionals. 2005. Accessed November 1, 2023. (Guidelines)
11. * American Academy of Pediatrics Committee on Injury, Violence, and Poison Prevention. Poison treatment in the home. Pediatrics. 2003;112(5):1182-1185. (Guidelines) DOI: 10.1542/peds.112.5.1182
14. American Academy of Pediatrics. Decontamination: disaster management resources. Patient Care. 2021. Accessed November 1, 2023. (Guidelines)
23. Adam H. Petechiae and purpura. Pediatr Care Online. 2021. Accessed November 1, 2023. (Quick reference) DOI: 10.1542/aap.ppcqr.396100
30. * Wu AH, McKay C, Broussard LA, et al. National Academy of Clinical Biochemistry Laboratory Medicine practice guidelines: recommendations for the use of laboratory tests to support poisoned patients who present to the emergency department. Clin Chem. 2003;49(3):357-379. (Guidelines) DOI: 10.1373/49.3.357
51. * American Academy of Clinical Toxicology European Association of Poisons Centres and Clinical Toxicologists. Position statement and practice guidelines on the use of multi-dose activated charcoal in the treatment of acute poisoning. J Toxicol Clin Toxicol. 1999;37(6):731-751. (Guidelines) DOI: 10.1081/clt-100102451
57. * Benson BE, Hoppu K, Troutman WG, et al. Position paper update: gastric lavage for gastrointestinal decontamination. Clin Toxicol (Phila). 2013;51(3):140-146. (Guidelines) DOI: 10.3109/15563650.2013.770154
58. * Krenzelok EP, McGuigan M, Lheur P. Position statement: ipecac syrup. American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. J Toxicol Clin Toxicol. 1997;35(7):699-709. (Guidelines) DOI: 10.3109/15563659709162567
135. American Association of Poison Control Centers. Track emerging hazards; laundry detergent packets. 2020. Accessed November 1, 2023. (Case report)
Subscribe to get the full list of 141 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: pediatric toxic ingestion, pediatric toxicology, poison control, Poison Control Center, toxidrome, urine drug screen, urine toxicology screen, ipecac, activated charcoal, whole-bowel irrigation, hemodialysis, acetaminophen, salicylates, anticholinergics, cholinergic agents, alcohol, digoxin, calcium-channel blocker, beta blocker, iron, opioids, sedative hypnotics, sulfonylureas, intravenous lipid emulsion, ILE, anion gap, osmolar gap, decontamination, hemodialysis, cannabis exposure, laundry detergent pod exposure, recreational street drugs
Mia Kanak, MD, MPH; Stacy Tarango, MD, FAAP; Deborah R. Liu, MD
Danielle Federico, MD, FAAP; Dan Quan, DO
December 1, 2023
December 1, 2026 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAP Prescribed Credits, 4 AOA Category 2-B Credits. Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 2 Pharmacology CME credits, subject to your state and institutional approval.
Pediatric Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Pediatric Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933
