

|
|
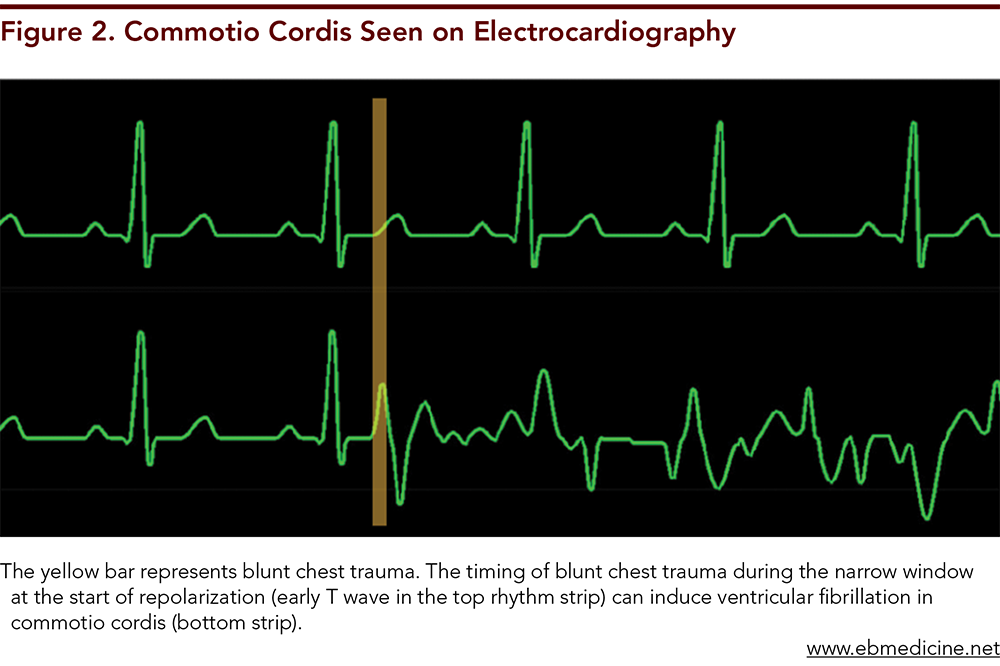
Pediatric chest trauma can present with a wide array of symptoms and with varying rates of morbidity and mortality. Children have unique thoracic anatomical and physiological characteristics, often necessitating diagnostic and management considerations that differ from management of blunt chest injury in adults. This review discusses diagnostic and treatment modalities for commonly encountered injuries in pediatric blunt thoracic trauma, such as pulmonary contusions, rib fractures, pneumothoraces, and hemothoraces. Rarely encountered but high-mortality injuries, including blunt cardiac injury, commotio cordis, tracheobronchial injury, and aortic injury, are also discussed.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
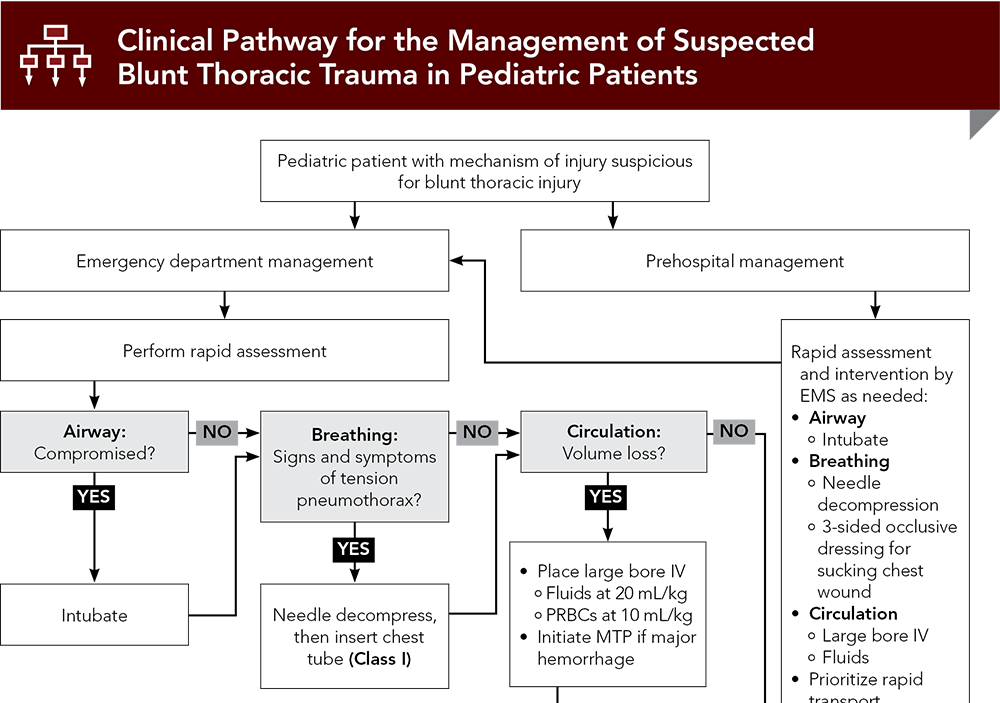
Subscribe to access the complete flowchart to guide your clinical decision making.
Subscribe for full access to all Tables.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
1. Office of Statistics and Programming. 10 leading causes of death by age group, United States--2010. Updated March 13, 2013. Accessed October 10, 2023. (US government statistical report)
4. * Black TL, Snyder CL, Miller JP, et al. Significance of chest trauma in children. South Med J. 1996;89(5):494-496. (Retrospective study; 1356 patients) DOI: 10.1097/00007611-199605000-00009
5. * Cooper A, Barlow B, DiScala C, et al. Mortality and truncal injury: the pediatric perspective. J Pediatr Surg. 1994;29(1):33-38. (Prospective study; 25,301 patients) DOI: 10.1016/0022-3468(94)90518-5
8. * Peterson RJ, Tepas JJ 3rd, Edwards FH, et al. Pediatric and adult thoracic trauma: age-related impact on presentation and outcome. Ann Thorac Surg. 1994;58(1):14-18. (Retrospective review; 2415 patients) DOI: 10.1016/0003-4975(94)91063-4
23. * Kessel B, Dagan J, Swaid F, et al. Rib fractures: comparison of associated injuries between pediatric and adult population. Am J Surg. 2014;208(5):831-834. (Retrospective cohort study; 6995 patients) DOI: 10.1016/j.amjsurg.2013.10.033
43. * McGwin G, Jr., Reiff DA, Moran SG, et al. Incidence and characteristics of motor vehicle collision-related blunt thoracic aortic injury according to age. J Trauma. 2002;52(5):859-865. (Retrospective study) DOI: 10.1097/00005373-200205000-00007
75. * Nagy KK, Krosner SM, Roberts RR, et al. Determining which patients require evaluation for blunt cardiac injury following blunt chest trauma. World J Surg. 2001;25(1):108-111. (Prospective study; 315 patients) DOI: 10.1007/s002680020372
106. *Markel TA, Kumar R, Koontz NA, et al. The utility of computed tomography as a screening tool for the evaluation of pediatric blunt chest trauma. J Trauma. 2009;67(1):23-28. (Retrospective review; 333 patients) DOI: 10.1097/TA.0b013e318184ba9a
Subscribe to get the full list of 107 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: blunt chest trauma, blunt thoracic trauma, blunt chest injury, blunt thoracic injury, blunt cardiac injury, pulmonary contusions, rib fractures, pneumothorax, hemothorax, blunt cardiac injury, commotio cordis, tracheobronchial injury, aortic injury
Glenn Goodwin, DO; Moshe Bengio, DO, MS, EMT-P; Christian B. Ryckeley, MD; Michelle N. Marin, MD
Stuart Bradin, DO, FAAP, FACEP; Paula J. Whiteman, MD, FACEP, FAAP
November 15, 2023
November 15, 2026 CME Information
4 AMA PRA Category 1 Credits™, 4 AOA Category 2-B Credits. Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 4 Trauma CME credits, subject to your state and institutional approval.
Pediatric Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Pediatric Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933
