
|
|
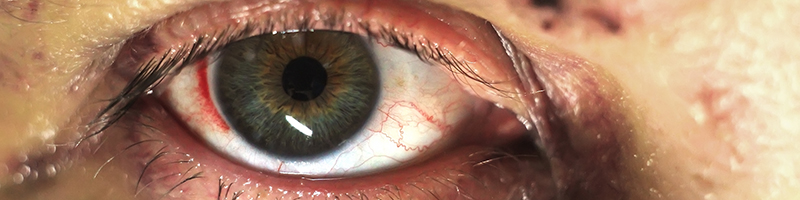
Ocular injuries are common in the emergency department, and they are the most frequent cause of noncongenital monocular blindness in children and adults. Systematic evaluation and management of ocular trauma patients will ensure these patients have the best chance for a favorable final visual outcome. This review provides evidence-based recommendations for the diagnosis, treatment, and disposition of patients with traumatic ocular injuries, including retrobulbar hemorrhage, traumatic hyphema, open globe injuries, ocular chemical burns, and corneal abrasions. The use of bedside ultrasound, antibiotics, cycloplegics, steroids, antifibrinolytics, and patching are also discussed.
Ocular injuries can be anxiety-provoking for both the patient and the emergency clinician. Traumatic eye complaints account for 3% of all emergency department (ED) visits in the United States,1 where eye injuries are the leading cause of monocular blindness nationwide.1-3 Eye injuries are also the most common cause of noncongenital unilateral blindness in the United States pediatric population.4
Fortunately, most eye injuries are minor and the overwhelming majority are not associated with significant morbidity.5 Even most ocular burns tend to be mild and inconsequential in the long term.6 In patients with mild injury, pain management and prevention of secondary infection are the mainstays of treatment. On the other hand, the multiply injured patient poses a particular clinical challenge because a proper eye examination may be difficult or impossible. This issue of Emergency Medicine Practice: Trauma EXTRA! reviews best-practice recommendations for the evaluation and treatment of ocular trauma patients based on the available evidence.
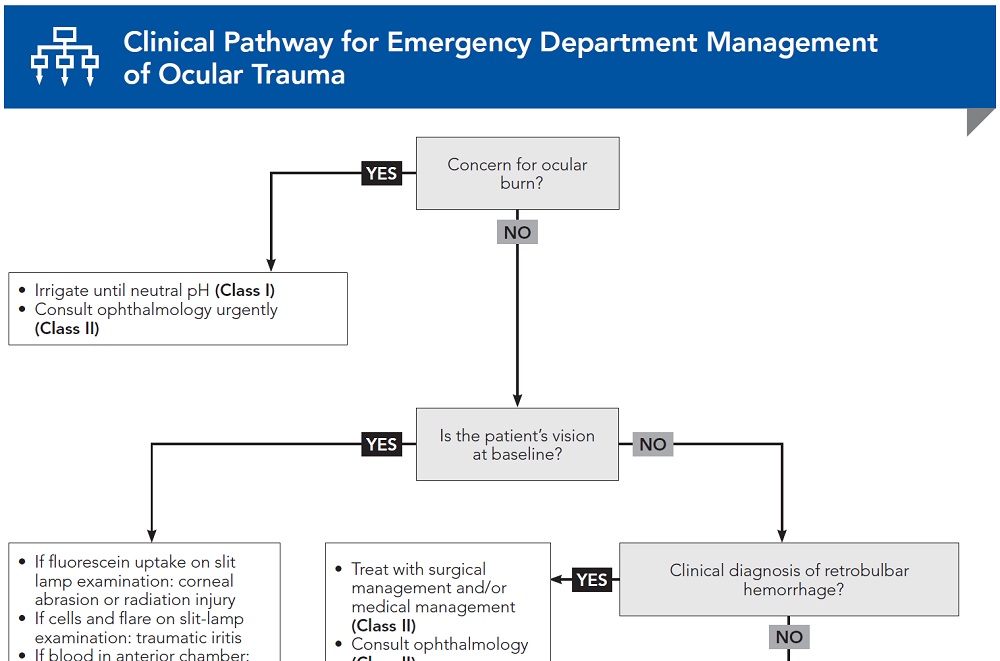
Subscribe to access the complete flowchart to guide your clinical decision making.
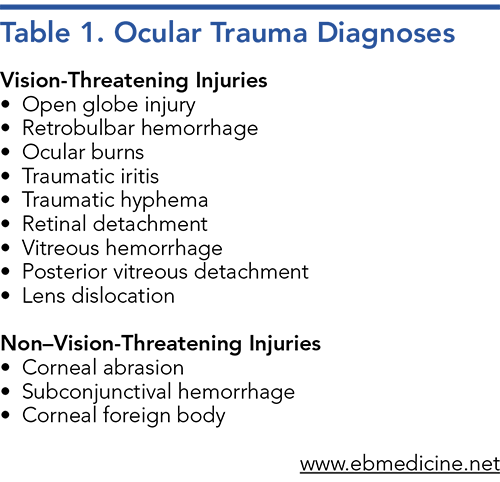
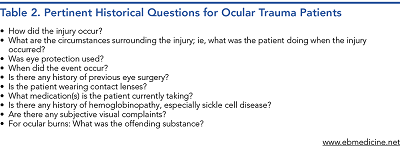
Subscribe for full access to all Tables and Figures.
Following are the most informative references cited in this paper, as determined by the authors.
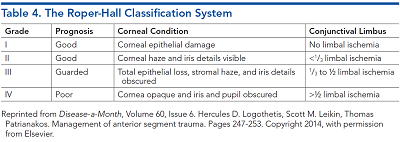
15. * Logothetis HD, Leikin SM, Patrianakos T. Management of anterior segment trauma. Dis Mon. 2014;60(6):247-253. (Review) DOI: 10.1016/j.disamonth.2014.03.004
22. * Brandt MT, Haug RH. Traumatic hyphema: a comprehensive review. J Oral Maxillofac Surg. 2001;59(12):1462-1470. (Review) DOI: 10.1053/joms.2001.28284
27. * Perry M, Moutray T. Advanced Trauma Life Support (ATLS) and facial trauma: Can one size fit all? Part 4: ‘Can the patient see?’ Timely diagnosis, dilemmas and pitfalls in the multiply injured, poorly responsive/unresponsive patient. Int J Oral Maxillofac Surg. 2008;37(6):505-514. (Review) DOI: 10.1016/j.ijom.2007.11.004
36. * Roque PJ, Hatch N, Barr L, et al. Bedside ocular ultrasound. Crit Care Clin. 2014;30(2):227-241. (Overview) DOI: 10.1016/j.ccc.2013.10.007
43. * Woreta FA, Lindsley KB, Gharaibeh A, et al. Medical interventions for traumatic hyphema. Cochrane Database Syst Rev. 2023;3(3):CD005431. (Cochrane review; 23 studies, 2969 patients) DOI: 10.1002/14651858.CD005431.pub5
63. * Calder LA, Balasubramanian S, Fergusson D. Topical nonsteroidal anti-inflammatory drugs for corneal abrasions: meta-analysis of randomized trials. Acad Emerg Med. 2005;12(5):467-473. (Meta-analysis; 11 trials) DOI: 10.1197/j.aem.2004.10.026
Subscribe to get the full list of 86 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: ocular trauma, ocular injuries, eye trauma, eye injuries, open-globe injury, corneal abrasion, ocular chemical burn, traumatic hyphema, traumatic iritis, proptosis, retrobulbar hemorrhage, corneal foreign body, lateral canthotomy
Emily Bae; Anne Messman, MD, MHPE; Kaushal Shah, MD, FACEP
Jennifer Maccagnano, DO, FACEP, FACOEP; Kelly P. O'Keefe, MD, FACEP
October 1, 2023
October 1, 2026 CME Information
4 AMA PRA Category 1 Credits™, 4 AOA Category 2-B Credits. Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 4 Trauma CME credits, subject to your state and institutional approval.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933