Table of Contents
About This Issue
Blast events can occur in any setting, bringing patients into the ED in waves that can overwhelm resources, with injuries that can range from benign to life-threatening. This issue reviews categories of blast mechanism, primary to quaternary, and the injuries to body systems that are likely to be seen in each category. Clinical pathways for management of injuries in each category are presented. In this issue you will learn:
The physics of how proximity to the blast affects body systems from blast wave, barotrauma, and fragmentation.
How the ears, lungs, abdomen, and brain are affected by spalling, implosion, and inertia.
The current protocols and algorithms used by prehospital providers in conjunction with ATLS®, FBI, Department of Homeland Security, and Federal Emergency Management Agency training.
How traditional trauma IV fluid resuscitation differs in patients with blast injury
What tympanic membrane rupture means: is it a biomarker for life-threatening injury?
Diagnosing pulmonary barotrauma: the most common fatal injury
The importance of re-assessments to spot development of delayed lung, brain, and abdominal injury
-
About This Issue
-
Abstract
-
Case Presentations
-
Introduction
-
Critical Appraisal of the Literature
-
Etiology and Pathophysiology
-
The Physics of Explosions
-
Bodily Effects of Blast Injury
-
Ears
-
Lungs
-
Gastrointestinal System
-
Brain
-
Differential Diagnosis
-
Prehospital Care
-
Principles and Strategies for Prehospital Management of Blast Injury
-
Cervical Spine Precautions
-
Transport
-
Emergency Department Evaluation
-
Initial Stabilization
-
History
-
Physical Examination
-
Ear, Nose, Throat, and Ocular
-
Cardiovascular
-
Respiratory
-
Abdomen
-
Skin
-
Neurologic
-
Psychiatric
-
Diagnostic Studies
-
Laboratory Studies
-
Imaging Studies
-
Ultrasound
-
X-Ray
-
Computed Tomography
-
Treatment
-
Special Populations
-
Pregnant Patients
-
Pediatric Patients
-
Elderly Patients
-
Controversies and Cutting Edge
-
Tympanic Membrane Rupture as a Biomarker
-
Permissive Hypotension in Resuscitation
-
Mental Health Effects
-
Pharmacologic Treatment
-
Critical Incident Stress Debriefings
-
Resources for Screening and Prevention of Posttraumatic Stress Symptoms
-
Disposition
-
Summary
-
Risk Management Pitfalls for Managing Patients With Blast Injuries in the Emergency Department
-
5 Things That Will Change Your Practice
-
Time- and Cost-Effective Strategies
-
Case Conclusions
-
Clinical Pathways
-
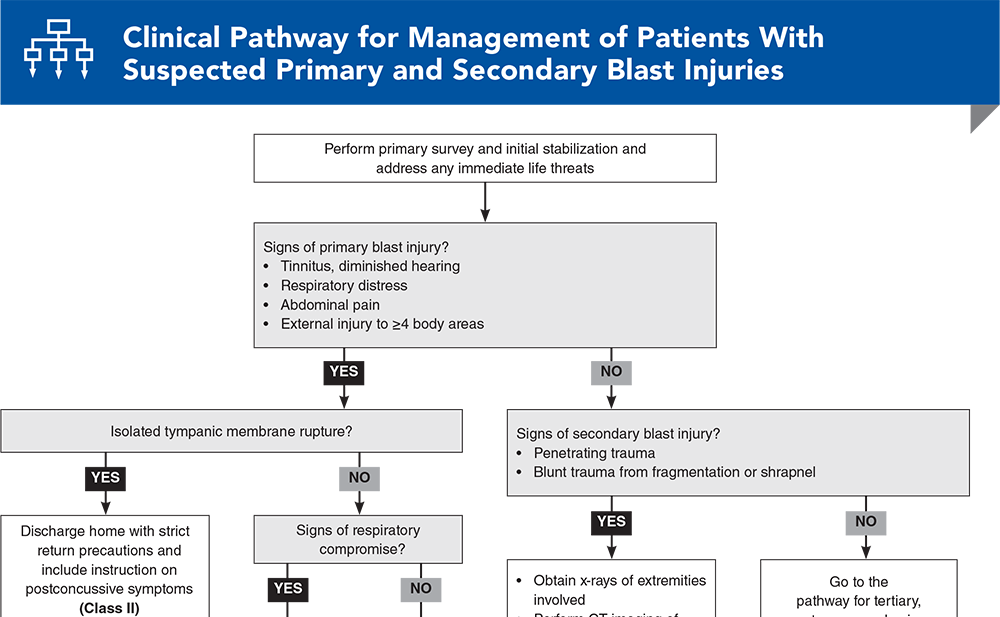
Clinical Pathway for Management of Patients With Suspected Primary and Secondary Blast Injuries
-
Clinical Pathway for Management of Patients With Suspected Tertiary, Quaternary, and Quinary Blast Injuries
-
Tables and Figures
-
References
Abstract
Managing patients with blast injuries can challenge emergency department operations, as patients can present in multiple waves, with occult or delayed injuries, and by personal transport, without standard prehospital care. Rapid and effective triage and evaluation includes approximation of blast proximity, determination of the category of blast – primary to quinary – and assessment of the body systems that are most likely to be injured from the type, location, and mechanism of the blast. This issue reviews the physics of the various types of explosions, how this affects the types of injuries that may be seen, and recommended treatments. Best-evidence recommendations are made for decision-making for observation, admission, or discharge.
Case Presentations
-
The patient arrives by personal vehicle.
-
She has no other complaints and no medical history. Her vital signs are: heart rate, 110 beats/min; blood pressure, 110/80 mm Hg; and oxygen saturation, 97% on room air.
-
You give her medication for pain control and a tetanus booster, and repair her extremity lacerations.
-
On re-evaluation, she says she feels better, though you wonder whether it is safe to discharge her or if there might be delayed sequelae of the blast that need to be watched for . . .
-
The boy says that he was crouching on the ground when the explosion occurred.
-
His heart rate is 84 beats/min; blood pressure, 100/82 mm Hg; and oxygen saturation, 98% on room air. He is complaining of bilateral tinnitus and diminished hearing. He denies any direct head trauma or loss of consciousness. His examination is remarkable for bilateral tympanic membrane rupture; otherwise, he has no other signs of traumatic injuries and no neurological deficits.
-
You wonder whether you should order a head CT, and if he‘s discharged, what instructions should be given to the parents...
-
The injured man, the bus driver, presents with shortness of breath. His heart rate is 118 beats/min, and blood pressure, 134/92 mm Hg. He is hypoxic at 87% on room air, with increased respiratory effort, and you note that he is bleeding from his ears bilaterally.
-
A police officer reports that the blast occurred in the back of the bus while the driver was in his seat.
-
Which category of blast injury likely caused this patient’s symptoms? What kind of injury pattern and pathophysiology would you be most concerned about?
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
Clinical Pathways
Subscribe to access the complete flowchart to guide your clinical decision making.
Tables and Figures
Subscribe for full access to all Tables, Figures and Appendix.
Buy this issue and
CME test to get 4 CME credits.
Key References
Following are the most informative references cited in this paper, as determined by the authors.
4. * Born CT, Briggs SM, Ciraulo DL, et al. Disasters and mass casualties: II. explosive, biologic, chemical, and nuclear agents. J Am Acad Orthop Surg. 2007;15(8):461-473. (Review) DOI: 10.5435/00124635-200708000-00003
7. * Halpern P, Tsai MC, Arnold JL, et al. Mass-casualty, terrorist bombings: implications for emergency department and hospital emergency response (Part II). Prehosp Disaster Med. 2003;18(3):235-241. (Review) DOI: 10.1017/s1049023x00001102
10. * Wolf SJ, Bebarta VS, Bonnett CJ, et al. Blast injuries. Lancet. 2009;374(9687):405-415. (Review) DOI: 10.1016/S0140-6736(09)60257-9
29. * Alfici R, Ashkenazi I, Kessel B. Management of victims in a mass casualty incident caused by a terrorist bombing: treatment algorithms for stable, unstable, and in extremis victims. Mil Med. 2006;171(12):1155-1162. (Retrospective editorial; 467 patients) DOI: 10.7205/milmed.171.12.1155
31. * Arnold JL, Halpern P, Tsai MC, et al. Mass casualty terrorist bombings: a comparison of outcomes by bombing type. Ann Emerg Med. 2004;43(2):263-273. (Systematic review; 8364 patients) DOI: 10.1016/s0196-0644(03)00723-6
45. * Nunziato CA, Riley CJ, Johnson AE. How common are civilian blast injuries in the national trauma databank, and what are the most common mechanisms and characteristics of associated injuries? Clin Orthop Relat Res. 2021;479(4):683-691. (Retrospective; 968,834 patients) DOI: 10.1097/CORR.0000000000001642
Subscribe to get the full list of 58 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords:













 678-366-7933
678-366-7933