
|
|
Patients who use supplemental herbal medications in an attempt to alleviate distress and/or enhance their lifestyles often present to the ED. Herbal products are readily available, having infiltrated our grocery stores, gas stations, truck stops, and convenience stores. The alternative medicine goal of treating the individual, not the disease, and requiring the patient to take responsibility for the healing process can make the use of herbal products appealing to a wide range of patients. "If it's natural, it must be safe," is often the adage patients abide by when self-treating disease.
Unfortunately, this canard can be dangerous. The problems of herbal poisoning and herb-drug interactions are both real and vitally important in the arena of emergency medicine. It is imperative that emergency physicians inquire about self-help modalities patients might be using on a daily basis. Not only is it important to ascertain whether the chief complaint might, in fact, be related to an herbal product, but herb-drug interactions must be explored as well.
This issue of Emergency Medicine Practice discusses what is currently known about herbal toxicology. It does not provide a comprehensive review of herbal medicine in general, but rather focuses on cogent data regarding those agents, particularly those that pose the greatest threat to the emergency patient population.
Herbal medicines are crude drugs of vegetable origin used for the treatment of disease states, often ones of a chronic nature, or to attain or maintain a condition of improved health. Because most herbal products in the United States are considered dietary supplements, they are not required to meet the standards for drugs specified in the Federal Food, Drug, and Cosmetic Act of 1938.
Herbal products can be marketed without any proof of testing for efficacy or safety. These products are governed by the Current Good Manufacturing Practice (CGMP) Regulations for foods, which are designed to ensure that dietary supplements are produced under sanitary conditions, but these regulations do not guarantee thepurity or efficacy of the product.
Packages containing herbals are not permitted to claim any ability to cure or prevent specific diseases, but are allowed to declare the ability to affect the body's structure or function in positive ways. The Dietary Supplement Health and Education Act of 1994 (DSHEA) assures the safety of these products and gives the herb manufacturer liberty to claim that their product "stimulates cardiovascular health" or "enhances sex drive," but opposes statements claiming "cures atherosclerosis" or "cures impotence."
Since 1999, the FDA implemented new rules for labeling that require supplement labels to provide a statement of identity, quantity of contents (number of capsules), structure-function claims, directions for use, fact panel, other ingredients, manufacturer, and distributor. In contrast to the United States, several European countries (Germany, France, Sweden) have implemented strategies for licensing herbal remedies, which allows premarketing assessment of the quality and safety of a product and facilitates postmarketing surveillance and product recalls.1
Presently in the US, there is the Adverse Reaction Monitoring System of the Food and Drug Administration, which enables the logging of clinical records, investigative reports, and autopsy findings in patients who may have been using or abusing herbal products.
Studies pertaining to herbal toxicology are for the most part limited to retrospective studies and case reports and series. No prospective clinical trials evaluating herbal toxicology were identified in our review of the literature.The National Center for Complementary and Alternative Medicine (NCCAM), which operates under the auspices of the National Institutes of Health (NIH), was established in 1998 to explore complementary and alternative healing practices, including herbal supplements. The NCCAM is funding most of the nation's current research aimed at increasing scientific knowledge about supplements. Among the substances that researchers are studying are ginger (as an anti-inflammatory), green tea (for its effects on heart disease), glucosamine hydrochloride and chondroitin sulfate (to see whether they relieve knee pain from osteoarthritis), echinacea (to see if it shortens the length or lessens the severity of colds in children), and ginkgo biloba (to determine whether it prevents or delays decline in cognitive function in people aged 85 years or older). However, most studies focus on the efficacy of various substances, rather than assessing issues relating to their toxicity.
American society is committed to herbal consumption. The herbal supplement business is literally a billion dollar industry and the popularity of herbal use has skyrocketed over the last decade. A survey of household herbal consumption in the United States revealed that 18.4% of all prescription users took herbal supplements concurrently, and out-of-pocket spending for herbal medication was $5.1 billion in 1997.2 In 1990, 2.5% of adults used an herbal medicine within the past year, compared to 12.1% in 1997.2 Hung et al determined a prevalence of 21.7% of herbal preparation use among patients presenting to an inner city ED.3 Gulla and Singer also found that 24% of their ED population had tried herbal supplements in the past.4 Rogers et al surveyed ED patients to assess risks of herbdrug interactions and found 14.3% regularly used herbal products while close to 80% did so while on concurrent prescription medications.5 Several studies in the primary care literature report similar trends. Herbal medication use ranges from 14% to 32% of patients surveyed, of whom at least half or more did not reveal this information to their physician.6,7,8
The top-selling herbal products that comprise the bulk of the supplement industry include: ephedra, ginkgo, St. John's wort, ginseng, garlic, echinacea, saw palmetto, grape seed extract, kava kava, evening primrose, goldenseal, cranberry, and valerian. Motivation to use these products is often related to availability and personal preference. 9
Additional indications for herbal remedies are for the treatment of depression, PMS, headaches, colds, decreased sexual stamina or sex drive, and lack of energy. Herbal products are also abused in order to induce euphoria, lose weight, stay awake, and build muscle. We managed a case of herbal abuse intended to alleviate the effects of ecstasy withdrawal. The patient found the specific recipe for this indication online and ordered the herbal products over the Internet.
Using herbal supplements can be compared to picking out candy from a box of chocolates; you never know what you're going to get. The lack of regulatory control results in considerable variation in the composition of an herbal supplement among manufacturers and lots, as well as mislabeling of actual content.10,11 The toxicity of the plant from which the herb is extracted may vary widely, depending on time of year or developmental stage at which the plant is collected.3 Adulterations, including heavy metals like lead, mercury, and arsenic, prescription medications, and other non-medicinal additives, have also been reported as risks to consumers.12 The inconsistency among products and the ever-present possibility of ingesting unexpected poisons place patients at unrealized potential for toxicity.
There are few well-controlled trials that examine the impact of prehospital care on the poisoned patient. Medics should perform basic stabilization measures, such as providing oxygen when needed, employing cardiac monitoring for those with unstable vital signs and cardiotoxic overdoses, and establishing venous access in those who may require fluids or life-saving medications. Gathering the patient's medications at the scene, including herbal medications, can aid in the diagnostic and management process upon arrival to the ED. The exact indications for these measures, however, have yet to be studied.
Ask all patients specifically whether they use any herbal supplements, in addition to the usual questions about medication use and other elements of the history. The patient's chief complaint may be related to herb use, herbdrug interactions, or adulterants in the herbal supplement. In other cases, the interaction between the emergency patient and physician provides a golden opportunity to educate the patient and possibly prevent future catastrophe resulting from an adverse reaction. For instance, patients can be warned to discontinue herbal supplements several weeks in advance of surgery, due to the possible bleeding risks associated with many herbal supplements.
Asking the patient if he or she is on any medications is rarely sufficient. Patients often feel vulnerable and are reluctant to tell a physician about their use of herbal products.3 In a study by Gulla and Singer, 70% of patients who had tried alternative therapies had not informed their physician of this practice.4
Knowledge of some of the more common herbal medications and their purported benefits (Table 1) may aid the practitioner in obtaining crucial elements of the history. For example, in patients who report being depressed or anxious, asking specifically whether they have been using St. John's wort or valerian may prove fruitful. Not only are adverse effects possible from use of these herbal supplements alone, but the combination of either of these with prescription medications also used for these conditions can present other risks, as discussed in subsequent sections.

Fortunately, adverse reactions to herbal medications are rarely immediately life-threatening (although exceptions have been documented). As with all ED patients, a sufficient physical examination based on the patient's presentation is necessary. There are no symptoms or physical examination findings that are pathognomonic for an adverse reaction to an herbal supplement. Indeed, given the wide range of herbs available, the potential findings are virtually limitless. Most presentations involve vague, nonspecific symptoms such as rashes, headaches, nausea, or altered sensorium that are typically difficult to assess. On occasion, however, serious complications, such as myocardial infarction, hemorrhage, seizures, or hepatotoxicity, can result from use of herbal supplements. (See Table 2.) While management is typically supportive, identification of herbal supplements as the cause of the patient's physical findings is essential to prevent future problems.

There are no toxicologic screens specific for herbal supplements. Diagnostic testing is usually determined on a caseby- case basis and is generally directed toward gauging possible complications, such as hepatotoxicity or cardiac damage, as discussed in later sections that cover management of specific herbal remedies.
The Ephedra species of several shrubs are often referred to by their Chinese name, ma huang. The pharmacologically active alkaloids include up to 90% ephedrine and various other forms, including pseudoephedrine and norephedrine. Because of its sympathomimetic properties, ephedra products are marketed as weight-loss aids, stimulants, energy boosters, and exercise enhancers. Many times, these products will include other herbal additives, caffeine, and various stimulants to increase efficacy, and often it is actually a concoction of herbs that patients are using. One study analyzing 20 ephedra-containing dietary supplements showed that alkaloid content was often inconsistent with corresponding label claims, and there were inconsistencies between various lots of the same products.10 Popular ephedrine-containing products include Metabolife, Ripped Fuel, Ultimate Orange, Purple Blast, and Yellow Jackets. Many of these supplements are advertised and sold over the Internet, in grocery and convenience marts, in addition to workout facilities and gyms. According to recent poison center data, 812 cases of ephedrine exposures were reported in 2001, with 3 associated deaths.13
Adverse effects from sympathomimetics like ephedra, which stimulate both alpha and beta receptors, include headache, nausea, vomiting, diaphoresis, insomnia, vetigo, agitation, psychosis, hypertension, tachycardia, palpitations, seizures, tremors, and rhabdomyolysis. Because of the pharmacology of ephedra, patients presenting after ingestions may present with toxicity affecting various organ systems, namely the cardiovascular (CV) system and the central nervous system (CNS). Ephedrine is rapidly absorbed and has an elimination half-life of approximately 5 hours.
Various cases are reported in the literature linking ephedra use with maladies coupled with significant morbidity and mortality. A previously healthy 19-year-old bodybuilder experienced 30 minutes of chest pain shortly after ingesting the recommended dose of Dymetadrine Xtreme and subsequently had a myocardial infarction.14 Many patients demonstrated similar adverse effects in 2 comprehensive studies evaluating possible CV and CNS manifestations after ephedra use.15,16 Haller and Benowitz independently reviewed 140 reports of adverse events related to ephedra use that were submitted to the Food and Drug Administration (FDA).15 Of the 140 cases, 31% were considered definitely or probably related to ephedra use, and another 31% were deemed to be possibly related.15 Age distribution in the "definitely" or "probably" related group ranged from 22 to 59 years.15 Duration of use ranged from 1 day to 1 year, and adverse events included subarachnoid hemorrhage, hemorrhagic strokes, arrhythmias, and cardiac arrest. 15 Permanent disability occurred in 7 out of 11 patients, and death in 3.15 Samenuk et al reviewed 926 cases of possible ma huang toxicity reported to the comprehensive database Adverse Reaction Monitoring System of the FDA from 1995 to 1997.16 Analysis of 37 of these patients indicated that ma huang appears to be temporally related to stroke, myocardial infarction, and sudden death. Underlying heart or vascular disease is not a prerequisite for related adverse events, and CV toxic effects are not necessarily directly proportional to massive dosing.16 Of the 37 patients, 11 experienced sudden death, 10 had myocardial infarction, and 16 patients suffered a stroke.16 These cases were interpreted to demonstrate a temporal relationship between ma huang and adverse cardiovascular events.16
Myocarditis-associated cardiomyopathy secondary to ephedra use has been reported.17,18 One 39-year-old patient with hypertension presented with a 1-month history of symptoms consistent with congestive heart failure.17 He had been using Herbalife, an ephedra-containing supplement, daily for 3 months prior to presentation and underwent a complete work-up, including cardiac catheterization reporting normal coronary arteries and a subsequent myocardial biopsy, which demonstrated myocyte hypertrophy in addition to an infiltrate consisting mainly of lymphocytes and eosinophils. After a 2-month Herbalife-free period, rebiopsy revealed no evidence of myocarditis, and within 6 months his ejection fraction had risen from 15% on initial presentation to 50%. The report suggested a temporal relationship between the patient's ephedra use and hypersensitivity myocarditis.17
Further cardiovascular toxicity is reported following herbal ecstasy abuse. Herbal ecstasy is a general term for a number of different preparations, usually containing both ephedra and caffeine sources, such as guarana or kola nut. Instead of being used for health, these products are ingested solely for the purpose of obtaining euphoria. One case series reported 5 patients who presented with insomnia, headaches, irritability, palpitations, dysrhythmias, hypertension, and tachycardia.19
Finally, other organ systems seem to be susceptible to adverse events associated with ma huang use. Acute hepatitis was reported in a previously well 33-year-old woman who presented with a several-week history of nausea, vomiting, abdominal pain, and jaundice.20 Symptom onset began several days after starting the supplement, and she was noted to continue her use for almost 3 weeks, stopping only after she noticed jaundice. The patient denied any significant past medical history, recent travel, or other medication use. Liver function tests were normal 2 years prior to admission. Her AST and ALT were 376 U/L and 832 U/L, respectively. After leaving the hospital in good condition, she restarted her regimen of ma huang use, which promptly resulted in a return of symptoms and doubling of her initial liver enzymes. This hospital course included a liver biopsy revealing diffuse hepatic necrosis, and an infiltrate of polymorphonuclear neutrophils, eosinophils, and plasma cells in the portal tracts and extending into the liver parenchyma. After discontinuing ma huang, clinical improvement was obtained and she was noted to be asymptomatic in 4 months.20 Another temporal association of ma huang-associated pathology includes renal lithiasis. A 27-year-old male with a history of a solitary right kidney and several episodes of renal colic was noted to ingest between 4-12 ProLift tablets a day to enhance his bodybuilding.21 Each tablet was reported to contain 170mg of ma huang. After stent placement and the subsequent passing of 2 stones, a stone analysis indicated 95% ephedrine metabolite. In addition, the reference laboratory indicated that they had analyzed over 200 stones with a similar profile as those from this patient.21
Recently, President Bush has supported the proposition to include on the label of ephedra-containing products a stern warning that cardiovascular and central nervous system disease may follow consumption. In addition, Suffolk County, New York has issued a ban on the selling of any ephedra supplements and placed significant fines to avert this practice. Because of the timeliness of this topic and the frequent reports of college and professional athletes suddenly dying with temporal relation to ephedra use, the emergency physician is on the front line when it comes to treating and educating patients who partake of ephedra.
A sound approach concentrating on the basics (airway, breathing, and circulation) is of foremost priority. For those who present either agitated and/or hypertensive, standard supportive care with adequate doses of benzodiazepines is prudent. Electrocardiograms are crucial in cases of associated chest pain or palpitations. Seizure activity not responding to benzodiazepines, may halt after the administration of barbiturates.22 Patients with headaches, specifically "worst headache of life" scenarios, deserve a conservative work-up, if clinically applicable, to rule out subarachnoid hemorrhage. Forgetting or deferring a lumbar puncture might result in significant morbidity and mortality in this patient population. Using ACLS guidelines and providing aggressive supportive care is paramount.
Ginkgo is the earth's oldest living tree species. Dating back over 200 million years, the ginkgo tree is also commonly referred to as the oriental plum tree or maidenhair tree. Popular among western medicine, ginkgo has been used for centuries for memory impairment in the elderly, asthma, and bronchitis. Currently, it is marketed to boost cognitive abilities (especially in Alzheimer's disease and other dementias) and to treat peripheral vascular disease, vertigo, tinnitus, altitude sickness, erectile dysfunction, and age-related macular degeneration.
The active components of ginkgo include flavonoids, which resemble folic acid and possess free radical scavenging properties, and terpenoids. Ginkgolide B, a potent inhibitor of platelet activating factor, is one such terpenoid of concern.
Adverse effects following acute exposure are usually limited to gastric upset, headache, and dermatitis. The fruit of the ginkgo has been known from ancient times to irritate the skin. Patients have been reported to experience erythema, edema, papules, and vesicles complicated by pruritus, which may be stinging or burning in character.23,24 A 63-year-old male was reported to experience a similar rash coupled with perioral and perianal burning, itching, and soreness just after eating 2 pieces of fruit that had fallen from a ginkgo tree.25 Ginkgolic acid, the primary allergen found in ginkgo, has also resulted in a progressive erythematous eruption over the face, neck, trunk, and extremities of a 66-year-old woman, after she took 2 60-mg doses of Trader Joe's ginkgo biloba supplement.26 Because of the structural similarity to the Toxicodendron spp, which includes poison ivy, a cross-allergenicity is thought to occur, resulting in dermal manifestation.
While it is unclear how ginkgo might incite seizures, several reports indicate seizures that appear temporally related to acute ginkgo ingestion. A previously healthy 36-year-old female consumed 70 to 80 ginkgo nuts during lunch for improved health and subsequently experienced nausea, vomiting, and generalized convulsions twice. After the acute toxicity resolved, the patient refrained from any further ginkgo products and was seizure free for 2 years, without need of antiepileptics.27 Likewise, a 2-year old child presented several hours after ingesting a large quantity of ginkgo seed and had an afebrile, 5-minute convulsion that ceased spontaneously.28 A constituent of the ginkgo seed, 4-methoxypyridoxine (MPN), is thought to potentially be responsible for the seizure activity and was actually noted to be elevated in the serum of the patient.28 Pyridoxine was administered to this patient, along with diazepam, which was speculated to prevent additional seizures that otherwise might have occurred.28 In addition to ginkgo seeds and nuts, tablets sold as supplements have also been implicated in precipitating seizures. Two elderly patients with known seizure disorders presented to the ED after several days of ginkgo use.29 Both patients were noted to be stable on anticonvulsants prior to presentation and the only new element in their medical regimens was the addition of ginkgo for the management of dementia. Several self-resolving seizures occurred during hospital admission, and it was noted months later, after stopping the supplement, that seizure activity had been nonexistent. 29 In addition to the actions of MPN, ginkgo flavonoids have been shown to exhibit GABAergic activity as partial agonists/antagonists at the benzodiazepine-binding sites.30 Because of the concern for seizure induction, ginkgo should not be used by individuals with known seizure disorders.
Ginkgolide B, a terpenoid and known platelet activating factor inhibitor, is thought to be responsible for the temporally related hemorrhages occurring after ginkgo ingestion. One healthy 33-year-old female presented with diffuse headaches worsening in severity over a 3-month period. She later experienced diplopia, nausea, vomiting, and right facial droop.31 An MRI revealed significant bilateral subacute subdural hematomas necessitating surgical evacuation. On further history, no trauma to the head was revealed, however, she described self-treatment with ginkgo biloba twice a day for 2 years. Aspirin and other nonsteroidal anti-inflammatory medications had not been used by the patient. She was noted, however, to have an abnormally prolonged bleeding time that normalized after the cessation of the herbal supplement. 31 Intracerebral bleeds and subarachnoid hemorrhages have also been temporally related to the use of ginkgo products. A 78-year-old female who was noted to be stable on warfarin for 5 years following a coronary artery bypass graft, presented with a left parietal hemorrhage after using ginkgo for the previous 2 months to enhance cognition.32 A previously healthy 56-year-old male was found confused at the wheel of his car and progressively demonstrated left hemiparesis, left hemianopsia, and left-sided neglect after taking ginkgo biloba as a general tonic 3 times per day for 18 months.33 In the ED, it was noted that the patient had a right parietal hematoma with considerable edema and midline shift.33 A 61-year-old male previously in excellent health presented to the ED with a 5-day history of headache, back pain, nausea, and sleepiness.34 He was noted to have a normal CT scan of the head, yet was diagnosed with a subarachnoid hemorrhage based on the lumbar puncture.34 His history was pertinent for a 6-month regimen of ginkgo 3-4 times per day. His clinical course was uneventful, and after discontinuing the herbal supplement he was also noted to have a reduction in his bleeding time.34 While there was no proof that the patient's supplement use caused the hemorrhage, the connection is suggested by the absence of other risk factors and the temporal association between increased bleeding time and ginkgo use.
Interestingly, other bleeding episodes have been noted to be temporally related to ginkgo use. A 70-year-old male presented to the ED with recurrent blurred vision in his right eye, at which time he reported a red discoloration through his cornea.35 He was found in the ED to have a fine stream of blood oozing into his anterior chamber. The bleeding tapered off after 5 minutes. He denied any recent trauma to the eye and had been on 1 aspirin tablet a day for 3 years following his coronary artery bypass surgery. The only new medicine he had been taking included ginkgo biloba 2 times per day for 1 week.35 After discharge, the patient stopped the ginkgo use, continued daily aspirin maintenance, and was noted to have no recurrence of bleeding over a 3-month follow-up period.35 Excessive bleeding postoperatively from the temporal use of ginkgo has also been reported.36 A 34-year-old male with a hemoglobin of 12.4 mg/dL after a laparoscopic cholecystectomy, subsequently dropped his hemoglobin to 5.4 mg/dL on post-op day 2. After being transfused successfully and questioned further, he admitted to using 2 ginkgo tablets per day.36
Since ginkgo is the number one selling herbal product, patients using ginkgo products are frequently presenting to EDs. While no deaths have been reported relating to ginkgo use, the emergency physician must be prepared to educate and intervene when necessary, in light of the reported temporal morbidity associated with its use. All patients with a history of seizures should be instructed to terminate ginkgo use. Any and all patients with histories or risks of hemorrhagic stroke should also be dissuaded from using ginkgo-containing products. For symptomatic patients with hemorrhage, primary treatment includes halting all ginkgo ingestion after a bleeding event is diagnosed. Blood typing for potential transfusion and consultation with the appropriate colleague (neurosurgery, general surgery, obstetrics, etc) is paramount. Post-op patients presenting to the ED should be routinely asked about herbal supplement use, especially those containing ginkgo. Educating the patient who is concurrently on anticoagulant medication may help avoid future catastrophes. Supportive care is the mainstay of therapy after acute or chronic ingestions of these products. Being cognizant of the above adverse effects will aid the clinician in the workup of the patient using or abusing ginkgo biloba.
Kava kava, also known as kava, ava, and kawa, is derived from Piper methysticum, which means "intoxicating pepper." It has a rich history dating back to the time of Captain James Cook's Pacific voyages in the late 1700s. Historically, kava has been an important part of ceremonial life for Polynesian cultures. Weddings, funerals, births, religious occasions, welcoming parties, and seasonal feasts have been the impetus behind kava consumption among these peoples. In addition to the ritual and social uses of kava, it has been used medically to treat several skin diseases, arthralgias, headaches, asthma, dysuria, and urethral discharge secondary to gonorrhea or chlamydia. Health food stores today advertise kava to relieve insomnia, induce deep sleep, enhance psychic powers, and promote a sense of sociability. Beverages and pills may contain this supplement alone or in combination with other herbal products. In 1998, it was estimated that the total retail sale of kava was $17 million.37 While 70-80% of kava is consumed in Polynesia, German citizens estimate 70 million daily uses.38 Kava consistently ranks within the top-ten selling herbs in the United States, and according to the most recent TESS data, US poison control centers received 336 calls regarding exposure to kava alone in 2001, with 1 death being reported.13
The main toxicities associated with kava use and abuse include dermatologic, neurologic, and liver dysfunction. Pharmacologically active constituents isolated from the plant are primarily a group of lipid-soluble alpha-pyrones called kavalactones. No specific dose response has been elucidated; however, there does seem to be a clear temporal relation between pathology and consumption. Kava's exact mechanism of action on the central nervous system has not been fully clarified. Hypotheses include a weak GABA-binding activity, blockade of serotonin and norepinephrine reuptake, sodium channel blockade, inhibition of monoamine oxidase type B, and blockade of dopamine receptors.45-50
Kava dermopathy has been described in Pacific Islanders who consume large concentrations of kava.39 The ichthyosiform eruption, likened to leprosy, has been noted as a scaling, white rash beginning on the head, with subsequent spreading to the feet, followed by exfoliation in the same direction. Proposed etiologies include interference with cholesterol metabolism, reduction in glandular secretions, accumulation of plant flavopigments or kavalactones, chronic allergic dermatitis, or a pellagra-like dermatosis.40-44 While chiefs and priests on pacific islands may consider the dermopathy as a sign of nobility and privilege, those who suffer from kava dermopathy obtain prompt reversal of effects with abstinence.
Kava has been shown to potentiate the effects of certain sedative hypnotics. Patients already on barbiturates or benzodiazepines are especially susceptible to CNS sedation if concomitant kava is ingested.51 In addition to sedation, choreoathetoid movement disorders have been reported after kava use. One patient was a 27-year-old Aboriginal Australian who presented 3 times with severe choreoathetosis involving his limbs, trunk, neck, face, and tongue musculature.52 The patient was noted to have an intact sensorium, and interestingly had resolution of symptoms after intravenous diazepam and a 12-hour observation. 52 Other dystonic reactions and extrapyramidal side effects were reported in 4 patients.53 Two of the patients noted sudden onset of dystonic reactions 90 minutes to 4 hours after their first dose, and the 2 other older patients (63-years-old and 76-years-old with Parkinson's disease) had an onset of movement disorder after several days of use.53 All 4 patients were successfully treated with anticholinergic medication.53 Another case involved a 45-year-old female who developed a severe Parkinsonism after 10 days of treatment with kava extract.54 This patient was prescribed kava to treat her symptoms of anxiety and for weight reduction. After a progressively worsening 3-month course of resting tremor, rigidity, gait disturbance, and lack of speech, it was discovered through her husband's keen observations that the onset of symptoms coincided closely with kava use.54 The patient, after an extensive work-up and treatment for depression, was treated with an anticholinergic medication. The majority of her symptoms faded and she was back to her daily routine at a 6-week follow-up visit.54 The authors comment that movement disorders induced by kava tend to appear with the first dose of medication and usually disappear quickly with drug withdrawal. Blockade of dopamine receptors is probably the mechanism of toxicity.54
Currently, there is a significant amount of discussion about kava and severe liver injury. Although liver damage appears to be rare, kava-containing products have been associated with liver-related injuries, including hepatitis, cirrhosis, and liver failure in other countries. In addition to reported adverse effects associated with kava use, the literature does report cases of hepatotoxicity. A 33-year-old female suffered malaise, loss of appetite, and jaundice after several weeks of kava use. 54 Her hepatitis was significant and the work-up was unable to pinpoint a causative factor. Liver biopsy revealed infiltrated portal tracts, bridging necrosis, destruction of interlobular bile ducts, and canalicular cholestasis. After 8 weeks of abstinence from kava, her liver enzymes returned to a normal level, and her recovery was uncomplicated.55 A 50-year-old male presented to the doctor with jaundice and admitted to using kava for 2 months.56 His liver function tests showed a 60-fold and 70-fold increase in AST and ALT, respectively. His clinical course was complicated by stage IV encephalopathy, respiratory failure, and subsequent liver transplant secondary to severe hepatic necrosis.56 The patient recovered uneventfully, as did a 14-year-old female after liver transplantation.57 This young girl was the firstreport of potentially fatal hepatotoxicity associated with the use of kava in a child. She was noted to presumably be taking the recommended dose of a commercially available kava preparation for 3 months to treat anxiety.57 The Food and Drug Administration recently issued a warning letter about 25 cases of serious liver toxicity in Germany and Switzerland, including cases of cirrhosis, hepatitis, and liver failure.58 Morbidity and Mortality Weekly Report ( http://www.cdc.gov/mmwr) also recently presented the investigation of 2 US cases of liver failure associated with kava-containing dietary supplement products and summarizes cases from Germany and Switzerland, commenting that a total of 11 patients had undergone subsequent liver transplantation.59 Several countries, including Germany, Switzerland, Canada, Australia, and France, have restricted the sale of kava-containing products based on the occurrence of hepatic adverse events and the documented hepatic toxicity following rechallenge with kava-containing products.60 In the face of kava use, genetic polymorphism may play a significant role in determining who might be subject to hepatic injury.
The approach to the patient after kava consumption is centered on supporting the airway and providing ventilation as necessary. For those not presenting with mental status decline, supportive care is appropriate, including an anticholinergic medication, like diphenhydramine, to treat dystonia and extrapyramidal movement disorders. Kava dermopathy warrants no medical treatment other than withdrawal of the supplement. High-risk patients with concomitant liver compromise should be warned about the possible adverse events of kava use and hepatic dysfunction. Kava supplementation should be withheld from all patients with known liver disease and those manifesting liver failure should be admitted with the understanding that liver transplantation has been an aggressive mode of treating those with severe hepatic dysfunction (ie, encephalopathy, coagulopathy, hepatorenal syndrome, and hemodynamic compromise). Emergency physicians should always consider questioning patients with evidence of hepatic injury about the use of herbal supplements, notably kava-containing products.
Hypericum perforatum, known commonly as St. John's wort, has been used to treat sleep disorders, anxiety, and especially depression. As the flower has historically been associated with healing powers and warding off the "evil spirits" of depression and mental illness, its name may have arisen as the flowers bloom around St. John's Day (June 24). Other traditional uses of the herb include treatment of excitability, neuralgia, fibrositis, sciatica, menopausal neurosis, and treatment of wounds. Not only is it one of the top-selling herbal products, its growth in sales has been enormous. Sales figures for the US alone in 1997 were reported to be close to $48 million, subsequently increasing by 2800% in just one year.61,62 United States poison centers received just over 300 calls pertaining to exposures to St. John's wort in 2001, 83 of which were intentional ingestions, 31 adverse reactions, and 26 with moderate outcomes.13
The major active constituents of St. John's wort include hyperforin, hypericin, a broad range of flavonoids, and tannins.63,64 The pharmacological mechanism of action has been debated and is not entirely clear. The proposed action of inhibiting monoamine oxidase (MAO) types A and B has been both supported and refuted by elaborate animal models.65-69 Other mechanisms of action supported by laboratory studies include binding to GABA and adenosine receptors, and inhibiting uptake of serotonin, dopamine, norepinephrine, GABA, and L-glutamate.70-73
While St. John's wort has been purported to have antimicrobial activity, its antidepressant actions are usually the incentive for use.74,75 Several studies have compared St. John's wort to either placebo or conventional antidepressants, including sertraline and imipramine, and have found that the Hypericum perforatum extract is not only effective when given to patients who are mildly to moderately depressed, but that its side-effect profile is such that patients tolerate St. John's wort very well.76-78 Because of these studies, ease of access, and effective marketing strategies, it is no wonder the emergency physician sees patients who are currently taking St. John's wort for depression and possibly various other reasons.
The adverse effects and toxicity associated with the use of St. John's wort are for the most part minor and include photosensitivity, gastrointestinal complaints, dizziness, and headache. However, CNS changes and the prospect of a serotonin syndrome in the right combination with other products is a potential that clinicians must be aware of. There are also numerous herb-drug interactions that must be taken into account when patients are seen in the ED.
Both topical and oral St. John's wort have been reported to result in sensitivity to sunlight, which has been referred to as hypericism.79 In addition, an erythroderma associated with St. John's wort has been described in a 44- year-old male who experienced a burning, erythematous rash beginning on the thighs and eventually including both sun-exposed and unexposed regions.80 The rash was noted to be bright red, hot, dry, and associated with fine scaling. No membrane involvement occurred and it resolved after discontinuing treatment and topical steroids.80
Several cases are reported in the literature supporting both hypomanic and manic episodes following the administration of St. John's wort.81-84 The patients from these reports were, for the most part, already diagnosed with a psychiatric condition, namely depression, and were reported to temporally become energetic, grandiose, irritable, hostile, aggressive, radically agitated, bizarre, hallucinating, pressured, and talkative after beginning St. John's wort at dosing according to product label. One patient, a 70-year-old female, with a history of an internal capsule infarct, Meniere's disease, and recurring depression, started taking St. John's wort to deal with the frustrations of her depression.84 After 2 weeks of therapy, she began to experience insomnia and hypomanic behaviors, including going on a $1,600 shopping spree.84
Another potentially serious adverse effect of St. John's wort ingestion is serotonin syndrome. Usually, the syndrome results from a combination of different agents with serotonin activity. When combining the inhibition of serotonin reuptake from St. John's wort with other serotomimetic agents, such as MAOIs or SSRIs, the result may look very similar to serotonin syndrome. Serotonin syndrome is a constellation of symptoms, including changes in mental status (agitation, confusion, restlessness, disorientation, or coma), autonomic instability (hypertension, tachycardia, tachypnea, diaphoresis, fever, or flushing), and neuromuscular changes (rigidity, myoclonus, tremor, hyperreflexia, or incoordination) in the face of excess serotonergic tone. 85 Several cases in the literature also reflect the temporal relationship between St. John's wort use and symptoms consistent with serotonin syndrome.86-88 Two of these cases report cardiovascular findings of hypertension and tachycardia in addition to mental status changes occurring right after dinner.86,88 One patient ingested red wine and cheese with his dinner, which leads one to be believe a tyramine reaction while taking St. John's wort is possible.86 Treatment for serotonin syndrome is mainly aggressive supportive care including cooling techniques and adequate benzodiazepine administration. While its ability to abate the symptoms of serotonin syndrome or change outcome is uncertain, some have reported the use of cyproheptamine (an antihistamine) 4 mg PO, which is thought to antagonize serotonin at its receptors.89,90
In addition to the possible adverse effects of St. John's wort use, multiple drug-drug interactions have been described in the literature. HIV patients, in particular, should think twice about its use, since plasma levels of protease inhibitors (indinavir, ritonavir, saquinavir) are reduced with concomitant St. John's wort use, thus potentially causing loss of HIV suppression.91 Other adverse reactions thought to occur via induction of various cytochrome enzymes by St. John's wort include lowering the levels of the following drugs; cyclophosphamide, warfarin, digoxin, oral contraceptives, theophyllin, and amitryptiline.92-95 In light of these drug interactions, patients could present with subtherapeutic levels of essential medications, breakthrough bleeding, or acute organ transplant rejection.96
Education is paramount when caring for patients who use St. John's wort. Supportive care is the mainstay of treatment of acute overdose. Patients must be encouraged to allow a sufficient lag time following the discontinuation of serotonergic agents before initiating therapy with St. John's wort, in order to avoid the potential induction of serotonin syndrome.
The Greek term Panax ginseng literally means "all-healing man root." This Asian native perennial herb has been a part of traditional Chinese medicine for over 2000 years. Taken as an adaptogen to enhance and/or restore normal well-being in the past, ginseng today has become a choice for those treating sexual dysfunction, cardiovascular disease, immune suppression, and cancer, in addition to enhancing cognitive and physical performance.97 While all parts of the plant contain active constituents (ginsenosides), the root is noted to be the most highly regarded. The commitment and dedication to ginseng use by Americans is evident from the amount of money spent yearly on the supplement. Even though studies have not established benefit for its touted indications, more than 6 million people use ginseng daily, and in the year 2000 alone, gross retail sales topped $60 million.98-100 Ginseng is available in a variety of preparations (root, extracts, capsules, teas, cigarettes) and is often sold in combination with other ingredients. The most recent poison center data indicated that 384 cases were reported in 2001, with no deaths attributed. 13
The pathophysiology is currently unknown.
Adverse reactions and toxicity from ginseng use are mainly limited to drug-drug interactions and chronic use of the supplement. A temporal relationship between manic episodes and ginseng use in patients with known psychiatric disorders has been reported.101-103 Two middleaged women with known diagnoses of affective disorders were noted to experience increased libido, hyperactivity, decreased need for sleep, irritability, aggressiveness, spending sprees, and "feeling like a bull," after several days of ginseng use for fatigue and depression.101-103 The symptoms abated after discontinuation of the herbal supplement and supportive care in a psychiatric facility. A 26-year-old male with no known psychiatric history was reported to experience bizarre behavior after a 2- month course of Chinese red panax ginseng as an energy booster.104 His history was consistent with ingesting the recommended dosage on the product label. There was no family history of bipolar disorder reported by the patient, who was hospitalized for treatment of his racing thoughts, pressured speech, grandiose ideas, flight of ideas, and loose associations.104 There are speculations whether ginseng itself is the actual culprit in cases of mania, or if in fact adulterants may be responsible.102 There are, however, several animal studies demonstrating neurotransmitter activity of ginseng that quite possibly could explain the mood disorders reported.105-107
Vaginal bleeding following ginseng use has been reported.108-110 Each case reports a temporal relationship between ginseng use and vaginal bleeding that subsided after discontinuation of the herb. One patient actually was noted to suffer hemorrhage in response to using ginseng facial cream purchased from China for dry skin during the winter months.109 In addition, other adverse effects include hypertension and cerebral arteritis.111,112 A severe headache in a 28-year-old female worsened 8 hours after drinking ginseng extract and was associated with vomiting and chest tightness.112 She was worked up and later found to exhibit a beading pattern of her anterior and posterior cerebral and superior cerebellar arteries consistent with arteritis. The hospital course was uneventful with resolution of her headache over the next week and a half, and there were no subsequent imaging studies.112
Chronic ginseng users have been reported to suffer from a variety of ailments.113 Siegel studied 113 patients who had been using ginseng for at least a month by interview and physical and psychological exams, which were then repeated at 6-month intervals for 2 years.113 The majority of patients used the supplement in PO preparations between 3 and 7 times per week. The catalogue of effects most commonly resulted in an elevation of mood, while 10 became euphoric, restless, agitated, and experienced insomnia. Other effects included diarrhea (47 patients), skin eruptions (33 patients), nervousness (25 patients), hypertension (22 patients), edema (14 patients), enhanced sexual performance (9 patients), and depression (6 patients).113 Siegel coined the term "ginseng abuse syndrome" and suggests that it mimics corticosteroid poisoning, with the only treatment required being withdrawal from the supplement and close attention to blood pressure.113
Other potential complications with ginseng use include herb-drug interactions. Ginseng-induced diuretic resistance was reported in a 63-year-old male who was admitted twice with weight gain and a history of ingesting a germanium-containing ginseng preparation. 114 The patient did respond to diuretics after withholding the supplement during his stay in the hospital, and he was subsequently discharged with a normal blood pressure and at his baseline body weight.114 Patients on digoxin may have a falsely elevated level if in fact they consume ginseng. A 74-yearold male was reported to have an elevated digoxin level at routine office visits that subsided after discontinuation of his Siberian Ginseng use.115 Headaches and tremulousness have been noted when combining ginseng with phenelzine.116,117 Finally, while an animal study shows no interaction between ginseng and warfarin, a case has been reported indicating that remaining adequately anticoagulated on warfarin may be difficult while concomitantly using ginseng.118
The approach to the patient after an acute overdose of ginseng is identical to that of other herbal products. Supportive care is of chief concern. Patients with psychiatric histories should be educated about the possible adverse effects of ginseng on lifestyle. Chronic users of ginseng should be warned about possible adverse affects reported. Pertinent drug interactions should be explored with appropriate patients. No specific antidote is available after consumption, and withdrawal of the agent is usually all that is necessary.
Derived from the root of the plant Valerian officinalis, valerian dates back to the time of Hippocrates as a treatment for digestive problems, flatulence, and urinary disorders. 119 The Latin word valere means "to be in health," and the more modern uses of the herb include treatment of insomnia, hypochondria, trembling, inner unrest, and excitability. Often, valerian is sold in health food stores combined with other herbal products. Coined "the valium of the 19th century," valerian appears to be used most of the time as a sleep-promoting agent.120 While France sells approximately 50 tons of valerian each year, US poison centers received 291 calls pertaining to exposure to the supplement in 2001, 44 of which had an adverse reaction reported, but no deaths.13
The activity of valerian is consistently attributed to 2 constituents: volatile oils and valepotriates.121 Purported mechanisms accounting for valerian's sedative-hypnotic effects include its interaction with GABA receptors and barbiturate-like CNS depressant effects.122-125 >From this information, one can envision the poisoned patient presenting with CNS sedation. Understanding the possible clinical findings associated with valerian use is essential for the emergency physician.
Toxicity to the liver from valerian has been discussed in the literature; however, the cases reported are weak and include other potential candidates (skullcap, asafetida, hops, and gentian) as possible etiologies.126 One other study failed to find any notable evidence of acute hepatitis in 23 patients after taking valerian.127 This same study did find that one of the main clinical problems experienced in 19 out of the total 23 patients was CNS depression.127 Willey et al reported that an 18-year-old college student presented to the ED 3 hours post-ingestion of up to 23.5 g of valerian root.128 Early after the overdose, the patient's first symptomatology included fatigue, in addition to abdominal and chest pain, tremor, and lightheadedness.128 The patient did well with supportive measures exclusively and had resolution of her effects within 24 hours of admission. 127 A case reported by Garges et al describes a 58- year-old male who was admitted to the hospital for a lung biopsy, and subsequently went into valerian withdrawal. 129 His delirium, tachycardia, and high-output cardiac failure abated after treatment with midazolam that was switched to clonazepam prior to discharge on hospital day 3.128 In light of the reversal of symptoms with benzodiazepines, and the fact that valepotriates have shown efficacy in attenuating symptoms of benzodiazepine withdrawal in rats, a withdrawal state from valerian must be kept in mind when one is entertaining sedative-hypnotic withdrawal
in a patient.130
No cases of serious poisoning from valerian are available in the published literature. Being cognizant of the sedative effects of the supplement will lead the physician to inquire of its use. Treatment is again supportive. Careful airway and ventilatory status is paramount in these patients. Aggressive supportive management coupled with conservative decontamination measures, like activated charcoal, is all that is required. Flumazenil, the reversal agent given in some isolated benzodiazepine overdoses, has not been reported useful in the face of symptomatic valerian poisoning. Teaching the emergency patient who takes prescription anxiolytics not to co-ingest valerian may in fact prevent a possibly dire herb-drug interaction.
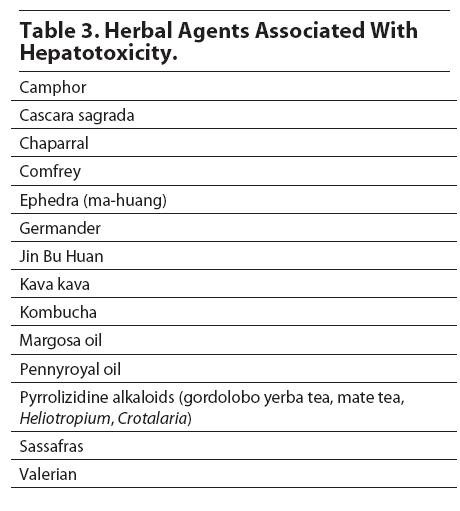
Derived from the root, leaves, and branches of Symphytum officinale, comfrey is the classic example of an herbal hepatotoxin. It is used for the treatment of fractures, tendon injuries, gastrointestinal tract ulcerations, and lung congestion. Comfrey has been shown to be an effective anti-inflammatory and healing agent; however, because it contains pyrrolizidine alkaloids, it may predispose a user to the development of veno-occlusive hepatic disease. Most of the toxicity has been experimentally demonstrated in animals.131,132 See Table 3 for a list of more common herbal hepatotoxins.133-140
While comfrey contains essential nutrients, it also contains potentially toxic pyrrolizidine alkaloids. The pyrrolizidine alkaloids are biotransformed in the liver to pyrroles, which exert their toxicity by binding to cellular macromolecules. 141 Pathologically, pyrrolizidine alkaloids cause a cirrhosis-like pattern and centrilobular necrosis. In one series, central veins were often unrecognizable. The veins that are still present show pronounced subendothelial edema with partial or complete luminal occlusion.142 The hallmarks of the disease are centrilobular hepatic necrosis and occlusion of the efferent veins. In some cases at biopsy, the hepatic veins were dilated and empty, but they were invariably associated with severely congested sinusoids in the pericentral zone.143
Comfrey is less toxic than other pyrrolizidine-alkaloids containing species (Senecio, Heliotropium and Crotolaria).143,144 Senecio and Crotalaria plants in the form of "bush tea" have been found in previous human cases to cause significant hepatotoxicity. 142
A patient who has consumed comfrey or another pyrrolizidine alkaloid may present with either hepatic insufficiency or fulminant hepatic failure. Liver enzymes, a complete blood count, electrolytes, renal function tests, and coagulation parameters should be obtained in all these patients. The key to making the diagnosis is to obtain a history of ingestion.
Treatment is essentially supportive, including rehydration, correction of coagulopathy, and observation for fulminant hepatic failure. Severe cases can be referred to a liver transplant unit, should the hepatic failure prove irreversible.
With the increasing use of herbal products by the general public, the potential for interaction with pharmaceuticals is great. Certain prescription medications have pharmacologic activity that can be accentuated by herbals. A recent survey identified a small group of ED patients who were at risk for such interactions.145 With the prevalence of herbal use increasing, it makes sense for the emergency physician to obtain a history of herbal use and to consider an herb-drug interaction. Patients will often not consider herbal remedies to be medications, so it is helpful to specifically question patients about all over-the-counter medicines, herbal medicines, dietary supplements, or alternative therapies they use. Table 4 presents some common examples of herb-drug interactions.145-158

Major problems with current herbal preparations are the lack of uniformity in preparation and in constituent concentration. Essentially one can't really know what is in the product being purchased.159 Also, another alarming and well-documented problem is the potential for adulteration with unlabeled active agents and toxic contaminants. In this and the following section on Chinese herbals, we willtouch on these issues that come up frequently in the medical literature.
Heavy metals are a common contaminant in many herbal products, particularly in Asian traditional remedies. Table 5 is taken from an investigation by Garvey documenting heavy metal adulteration.160
One of the first cases of lead contamination of an herbal product was reported in 1977.161 A 59-year-old woman was taking an herbal remedy for arthritic pains for 4 months. She developed anemia with basophilic stippling and had a whole blood level of 90 mcg/dl. An Indian herbal medicine prescribed for weakness caused lead poisoning (lead level of 153 mcg/dl) when taken chronically. Lead has been reported to be a contaminant in both Indian and Chinese herbal products. It has also been reported as an adulterant in folk medicines from Oman, Mexico, Pakistan and other Middle Eastern countries.162 Azarcon (lead tetroxide) and greta (lead oxide) are 2 Mexican remedies that have caused lead poisoning. They are fine powders that contain from 70-90% lead. Having been used for the treatment of colic, diarrhea, and other gastrointestinal illnesses, they have been responsible for numerous cases of lead poisoning.163-164 A Hmong folk remedy used by refugees from Northern Laos has caused similar lead toxicity. The remedy, known as "pay-loo-ah," is a red and orange powder that also contains a high concentration of lead.165
Thallium poisoning has resulted from a Chinese herbal medication, "Nutrien," purchased in the United States. This toxicity manifested as alopecia and sensory neuropathy.166
Cosmetics have been documented as a source of heavy metal poisoning. Surma is a source of lead expo- sure. Surma is a fine powder that looks like mascara but is applied to the conjunctival surfaces of eyelids. The word Surma is derived from the Urdu word for antimony. Since antimony is scarce, lead has been substituted and has caused cases of elevated lead concentration.167 This substance, also known as kohl, is used in Israel and Middle Eastern countries. Surma has been documented to contain up to 86% lead sulfide.168
Ayurveda is a traditional system of medicine practiced mostly in India, Sri Lanka, Bangladesh, Pakistan, Burma, Bhutan, Tibet, and Mongolia. Ayurvedic preparations can contain herbal products, animal products, metals, and minerals. Like other traditional medicines, their preparation is unregulated. A Croatian study found a wide range of lead content (from 0.9-72,990 mcg Pb/g) in Ayurvedic metal-mineral tonics.169
Other traditional Indian herbal remedies have been reported to contain various heavy metals: lead (aphrodisiac, anti-diabetes medication, Mahayograj Guggul), arsenic (eczema remedy), and mercury (eczema remedy, arthritis remedy). (See Table 5.)170,171

Asian patent medicines may contain products such as herbs, plants, animal parts and minerals that are formulated into tablets, pills, or liquids. Many of these ingredients will not be contained on the label.172 Ko conducted an analysis of 260 Asian patent medicines that were collected from California herbal stores. Seventeen of 243 products contained undeclared pharmaceuticals. The most common ingredients were ephedrine, chlorpheniramine, methyltestosterone, and phenacetin. A total of 251 products were analyzed for lead, arsenic, and mercury. Twenty-four products contained lead in at least 10 parts per million, 36 contained arsenic, and 35 contained mercury. In total, 83 of 260 products contained undeclared pharmaceuticals or heavy metals, and 23 had 1 or more adulterant.172 This illustrates the danger and lack of standardization of these products.
Six cases of herbal poisoning of patients in Hong Kong, Taipei, and Kuala Lumpur were described in patients taking wei ling xian and pao tung hua that were contaminated with podophyllum and Datura metel, respectively. The 2 patients ingesting the contaminated wei ling xian developed encephalopathy or neuropathy. Pao tung hua is prescribed for UTIs, mumps, enteritis, dysentery and conjunctivitis. In the other 4 cases, the flowers were contaminated with Datura metel, which is an anticholinergic preparation causing drowsiness and confusion. 173
Vanhaelen analyzed 12 batches of so-called Stephania tetrandra and found that all but 1 batch contained the contaminant aristolochic acids, not the expected tetrandrine. In Belgium 70 cases of progressive interstitial fibrosis of the kidney (30 end-stage) have been identified. The suspected toxin is the aristolochic acids found as a contaminant. 174
Pesticide contamination is an additional concern in herbal remedies. These natural products can assimilate heavy metals. In an investigation of 21 over-the-counter ginseng products, 5 samples contained chlorinated pesticides exceeding 100 ppb. None of the samples tested contained detectable quantities of chromium, mercury, or arsenic.175
Undeclared pharmaceuticals are often found in Asian patent medications. Black balls from China have been purported to contain "stealth steroids." The contents of these products are not listed on the packaging. One investigation documented the presence of prednisone and indomethacin in all samples of herbal pills used for rheumatoid arthritis symptoms.176,177 "Chinese black balls" are sold as a treatment for arthritis, liver and kidney ailments, muscle aches, and miscellaneous indications under the names of "Miracle Herb," "Tung Shueh," and "Chuifong Toukuwan." These products contain diazepam and mefenamic acid. There are cases reported of altered mental status and significant gastrointestinal bleeding from these agents.178 In addition, arsenic and mercury contamination has also been reported in traditional Chinese herbal balls.179
One Chinese remedy, Chuifong Toukuwan, has been found to contain phenylbutazone, aminopyrine, indomethacin, and hydrochlorothiazide.180,181 A Chinese herbalist prescribed "Golden Seal Extract" for a patient's dental pain. The product was contaminated by aminopyrine.182 Chuifong Toukuwan, a Chinese arthritis remedy, was found to contain aminopyrine and phenylbutazone not declared on the packaging. 183 Four patients taking Chinese herbal medicines containing aminopyrine and phenylbutazone (both known to cause agranulocytosis) for musculoskeletal pain developed life-threatening infections with sepsis and death in 1 patient.184 Phenylbutazone in one herbal medication billed as a "natural herbal remedy" led to aplastic anemia in a 12-year-old Asian boy.185
Hypoglycemia is a potential consequence of certain Chinese proprietary medicines (CPMs; also known as Chinese patent medicines). A Malaysian man developed recurrent hypoglycemia after taking a product known as "ZhenQi" for diabetes. Analysis demonstrated the presence of sulfonylurea glibenclamide.186
When obtaining a history of Asian patent medication use, the emergency physician should consider not only the pharmaceutical effects, but also the potential toxicity of adulterants and undeclared pharmaceutical agents (Table 6).

Traditional Chinese medicine is growing in popularity. Along with a large number of Chinese Americans, CPMs are in wide use among other segments of the US population. The emergency physician should be aware that these medications have similar problems as discussed with other herbals. There is wide variation in preparation, and there can be significant contamination (see section on adulteration).
In a New York City survey serving a large ChineseAmerican population, 43% of those ED patients had used a Chinese therapy within 1 week of their ED visit. In addition, 17% of those patients saw both a Western and a Chinese practitioner.187
The preparations reported to be used by those patients included: ginseng (Panax ginseng), Lycium (Lycium chinense), licorice (Glycyrrhiza uralensis), peony (Paeonia albiflora), tang kuei (Angelic sinesis), and miscellaneous herbal mixtures.187
In a study conducted in Hong Kong, 71 individuals took overdoses containing CPMs. The majority of cases were asymptomatic, but 28 had symptoms of minor gastrointestinal irritation or salicylate poisoning. (See Table 7.) One patient had serious salicylate toxicity after taking Hung Far Oil (Red Flower Oil).188

Other interesting overdoses of Chinese medications that lead to toxicity are Jin Bu Huan, Tripterygium wilfordii hook, and aconitine.
Three unrelated overdoses of Jin Bu Huan in toddlers led to life-threatening bradycardia, CNS, and respiratory depression. Jin Bu Huan is billed as a "particularly good remedy for the patient suffering from insomnia due to pain." Jin Bu Huan contains levo-tetrahydropalmatine, a substance extracted from the plant genus Stephania.189 Subsequently, 3 cases of acute hepatitis were described in 3 adults taking Jin Bu Huan.190
Tripterygium wilfordii hook F (TWHF) is a Chinese herbal medicine that is applied externally for arthritis. Recently it has been found to possess immunosuppressive effects that may be useful for autoimmune disorders. A healthy 36-year-old man developed profuse vomiting, diarrhea, leukopenia, renal failure, shock, and death after ingesting an extract of TWHF.191 As is the problem with many of these medicines, the purity and concentration of the active agents is difficult to assess, and can therefore present danger to patients taking them.
Some CPMs contain "chuanwu" and "caowu," originating from the roots of some Aconitum species. These plants are known to have potent anti-inflammatory effects, but are also potential cardiac toxins.192 One case series of 8 patients documented paresthesias, gastrointestinal complaints, hypotension, and dysrhythmias.192 Another series of 3 cases led to fatal tachyarrhythmias.192
As with the management in these patients, disposition in cases of herbal toxicity is largely case-dependent. In the majority of cases, clinically stable patients with benign physical examinations, and who are deemed to be at low risk for complications, can be safely discharged with good follow-up instructions. In cases of hepatotoxicity, cardiovascular compromise, or other serious sequelae, admission and/or specialist referral may be necessary. Patient education particularly concerning possible future herband/or herb-drug reactions is of special importance. (See Table 8.)

The use of herbal remedies is exploding in the general population. Many of these preparations are manufactured with variable levels of quality control. These products have a myriad of pharmacological and toxicological properties. It is useful for the practicing emergency physician to have familiarity with some of the more common herbal products: ephedra, ginkgo biloba, kava, St. John's wort, ginseng, valerian and comfrey. One should be aware of the potential for herb-drug interactions, and appreciate the risk of the presence of adulterants or undeclared pharmaceuticals in herbal products. Finally, in the ED, we should obtain a history of use of herbal or other alternative therapies, in order to routinely recognize these potential problems. (See Table 9 for a listing of Web sites that can provide the most up-to-date information and advisories for the ED physician.)

1. "Of course it is safe; it's herbal. It's natural."
This is a common misconception among not only the lay public, but with health care professionals as well. It is important that emergency physicians become familiar with the risk in the formulations and actual contents of herbal preparations.
2. "Of course it's safe. You can buy it at the mall!"
As above, just because it's widely available does not guarantee its safety. As the regulations for review for herbal products and dietary supplements come under greater scrutiny, we will probably in the future find fewer of these problem products available for purchase at the mall.
3. "It's not a medication; it's a supplement."
We must remember that supplements are not regulated and tested by the FDA. "Supplements" are not subjected to rigorous testing, as are "pharmaceuticals."
4. "No, I didn't consider an interaction of that preparation with the patient's medications."
As reviewed in this article, many herbal medications can interact with a variety of medications. It is helpful for clinicians to be aware of the more common ones.
5. "I told my patient to go see an herbal medicine practitioner."
As with some alternative therapies, herbal medicine does provide relief to some patients. However, if not trained in this area, it is wise not to recommend products that are not part of conventional medical training. This is a potential area for legal exposure for practitioners.
6. "I didn't consider an herbal preparation as a cause for the patient's liver failure."
Some herbal preparations can lead to hepatic failure. It is useful to take the history of herbal medication consumption and consider it in the differential diagnosis for hepatic failure.
7. "It was just mascara."
Mascaras and other cosmetics have been documented to be sources of heavy metal (lead) exposure. It is useful to be aware of such risks.
8. "I said it's probably fine to keep taking that Chinese herbal remedy for that nonspecific abdominal pain."
Again, unless trained as an herbalist, one should avoid making recommendations about the use of herbal medications. Medications in general can mask a serious clinical condition. Also, some Asian patent medicines can be a source of lead exposure, which can actually cause crampy abdominal pain as a sign of lead poisoning.
9. "I thought it was a simple GI bleed."
It is essential to recognize that herbal preparations may be the precipitating factor in bleeding episodes. Ginkgo has been well documented to cause bleeding problems, including GI, and intracranial hemorrhage. To prevent further episodes of bleeding in the future, it is key to educate the patient of this side effect.
10. "I don't take a history for herbal medication."
Take it! As this review article points out, there are many toxic issues involved with herbal medicines.
1. Ask specifically about the use of herbal supplements.
Not only is the use of herbal supplements a growing, billion-dollar industry in the United States, but it can also be associated with a variety of complaints like headache, rashes, and nausea that can be notoriously difficult to work up.
2. Don't count on patients to volunteer information about the use of herbal supplements.
Patients may assume that physicians will disapprove of the use of herbs or they may assume that "natural means safe," and that therefore herbal supplement use isn't worth mentioning. Soliciting a patient's medication history could be more effective if you ask specifically about prescription medications, over-the-counter medications, and herbal or other supplements, rather than just asking for a list of "medications."
3. Keep an eye out for self-treatment with herbs when a diagnosed condition exists or the patient is on a prescribed medication that is often treated with herbs.
Is your patient on MAOIs also self-treating with St. John's wort? Is your patient taking valium and valerian at the same time? You might not know unless you ask. These examples and others can produce dangerous herb-drug interactions.
4. Educate patients about the potential drawbacks of herbal supplement use.
The ED encounter can be a golden opportunity to prevent future problems. (See also Table 8.)
|
|
|
|
 |
|
|
|
|
|
|
|
|
|
|
|
|
Evidence-based medicine requires a critical appraisal of the literature based upon study methodology and number of subjects. Not all references are equally robust. The findings of a large, prospective, randomized, and blinded trial should carry more weight than a case report.
To help the reader judge the strength of each reference, pertinent information about the study, such as the type of study and the number of patients in the study, will be included in bold type following the reference, where available.
Sean Bryant; Steven Aks
January 1, 2005
Emergency Medicine Practice • CONTINUE READING
Access every issue, our complete clinical pathway library, and earn up to 190 CME credits with an annual subscription.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933