

|
|
Low back pain is a common presentation in the emergency department, and determining whether the cause is benign or life-threatening can be challenging. A systematic strategy for the history and physical examination can help reduce unecessary imaging, and an evidence-based approach will inform safe and effective pain management recommendations. This issue reviews the evidence on red flag signs and symptoms for low back pain, current diagnostic studies recommendations, and best-practice treatment and disposition strategies.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
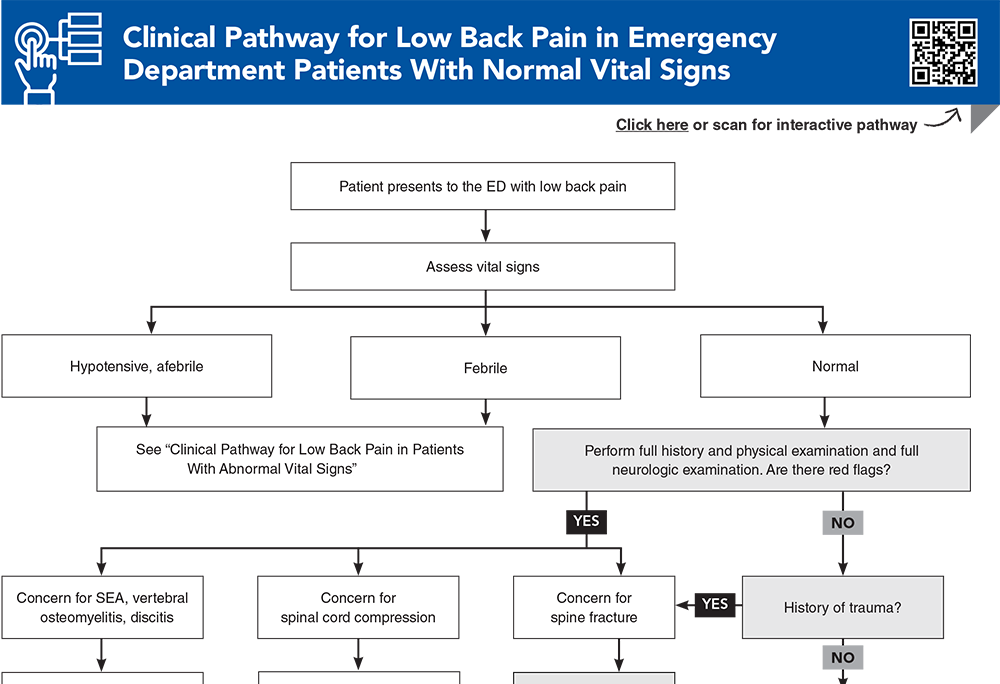
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
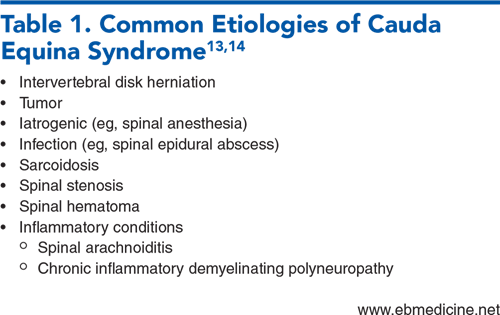
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
20. * Galliker G, Scherer DE, Trippolini MA, et al. Low back pain in the emergency department: prevalence of serious spinal pathologies and diagnostic accuracy of red flags. Am J Med. 2020;133(1):60-72. (Systematic review; 22 studies) DOI: 10.1016/j.amjmed.2019.06.005
25. * Friedman BW, Mulvey L, Davitt M, et al. Predicting 7-day and 3-month functional outcomes after an ED visit for acute nontraumatic low back pain. Am J Emerg Med. 2012;30(9):1852-1859. (Prospective study; 556 patients) DOI: 10.1016/j.ajem.2012.03.027
29. * Dionne N, Adefolarin A, Kunzelman D, et al. What is the diagnostic accuracy of red flags related to cauda equina syndrome (CES), when compared to magnetic resonance imaging (MRI)? A systematic review. Musculoskelet Sci Pract. 2019;42:125-133. (Systematic review; 7 studies) DOI: 10.1016/j.msksp.2019.05.004
46. * Chou R, Fu R, Carrino JA, et al. Imaging strategies for low-back pain: systematic review and meta-analysis. Lancet. 2009;373(9662):463-472. (Meta-analysis; 7 studies) DOI: 10.1016/S0140-6736(09)60172-0
50. * Downie A, Hancock M, Jenkins H, et al. How common is imaging for low back pain in primary and emergency care? Systematic review and meta-analysis of over 4 million imaging requests across 21 years. Br J Sports Med. 2020;54(11):642-651. (Meta-analysis; 45 studies) DOI: 10.1136/bjsports-2018-100087
70. * van der Gaag WH, Roelofs PD, Enthoven WT, et al. Non-steroidal anti-inflammatory drugs for acute low back pain. Cochrane Database Syst Rev. 2020;4(4):CD013581. (Cochrane review; 32 trials) DOI: 10.1002/14651858.CD013581
78. * Friedman BW, Dym AA, Davitt M, et al. Naproxen with cyclobenzaprine, oxycodone/acetaminophen, or placebo for treating acute low back pain: a randomized clinical trial. JAMA. 2015;314(15):1572-1580. (Randomized controlled trial; 323 ED patients) DOI: 10.1001/jama.2015.13043
86. * Ashbrook J, Rogdakis N, Callaghan MJ, et al. The therapeutic management of back pain with and without sciatica in the emergency department: a systematic review. Physiotherapy. 2020;109:13-32. (Systematic review; 26 articles) DOI: 10.1016/j.physio.2020.07.005
Subscribe to get the full list of 113 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: herniation, compression, epidural, hematoma, abscess, myelitis, sciatica, immunocompromise, cauda equina, stenosis, skip lesion, opioid, NSAID
Kevin Molyneux, MD, MPH; Sabena Vaswani, MD, MPH
John Rozehnal, MD; Randy Sorge, MD, FACEP
November 1, 2024
November 1, 2027 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933