
|
|
Status epilepticus is a neurological emergency requiring prompt intervention by emergency clinicians, as delays can lead to significant morbidity and mortality. Etiologies include acute causes such as electrolyte imbalance, infection, drugs, and acute strokes, as well as chronic causes such as remote brain injury, progressive epilepsies, and brain tumors. This issue presents evidence for an algorithmic approach to status epilepticus, from managing underlying causes and administering initial benzodiazepines, to second-line antiseizure agents, and escalating to intravenous anesthetics for refractory cases. Disposition for patients in status epilepticus includes inpatient care tailored to the patient’s clinical needs, and appropriate follow-up.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
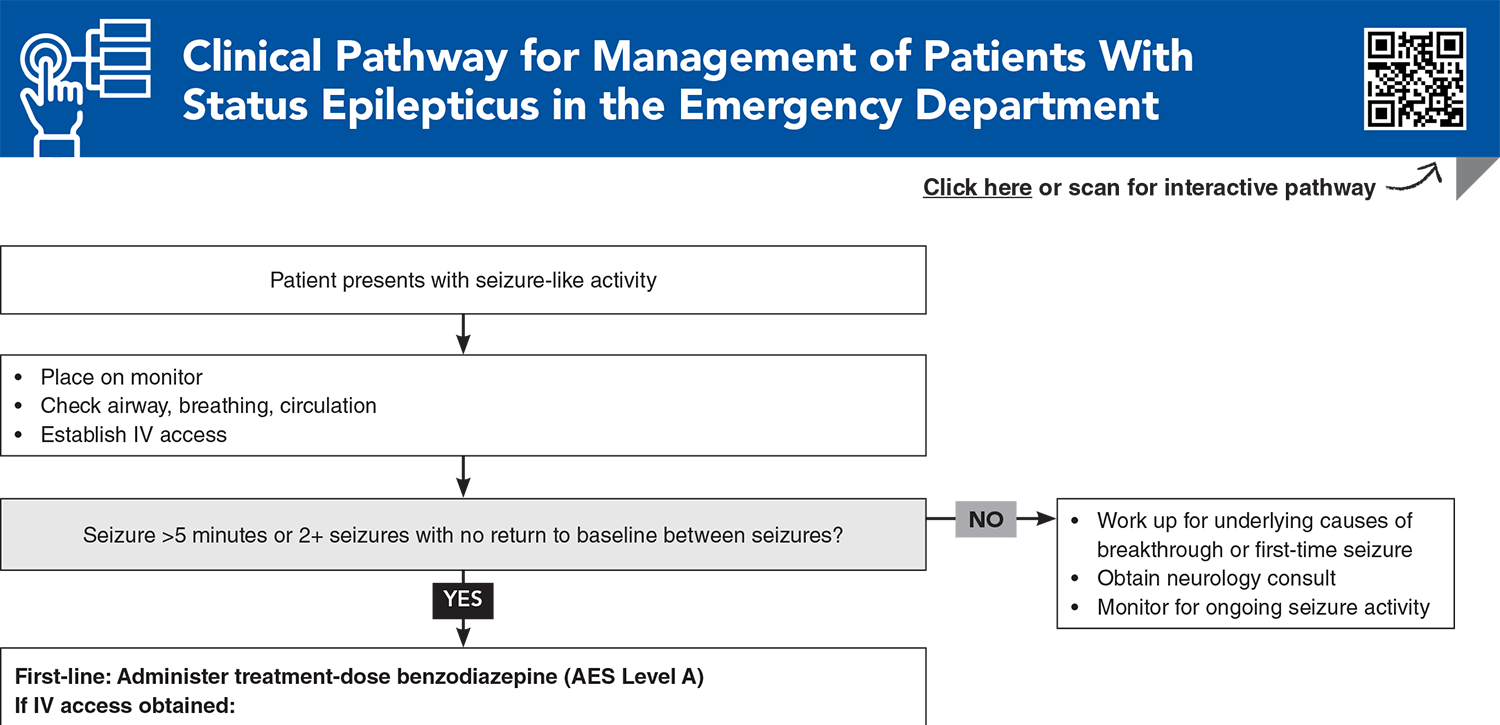
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
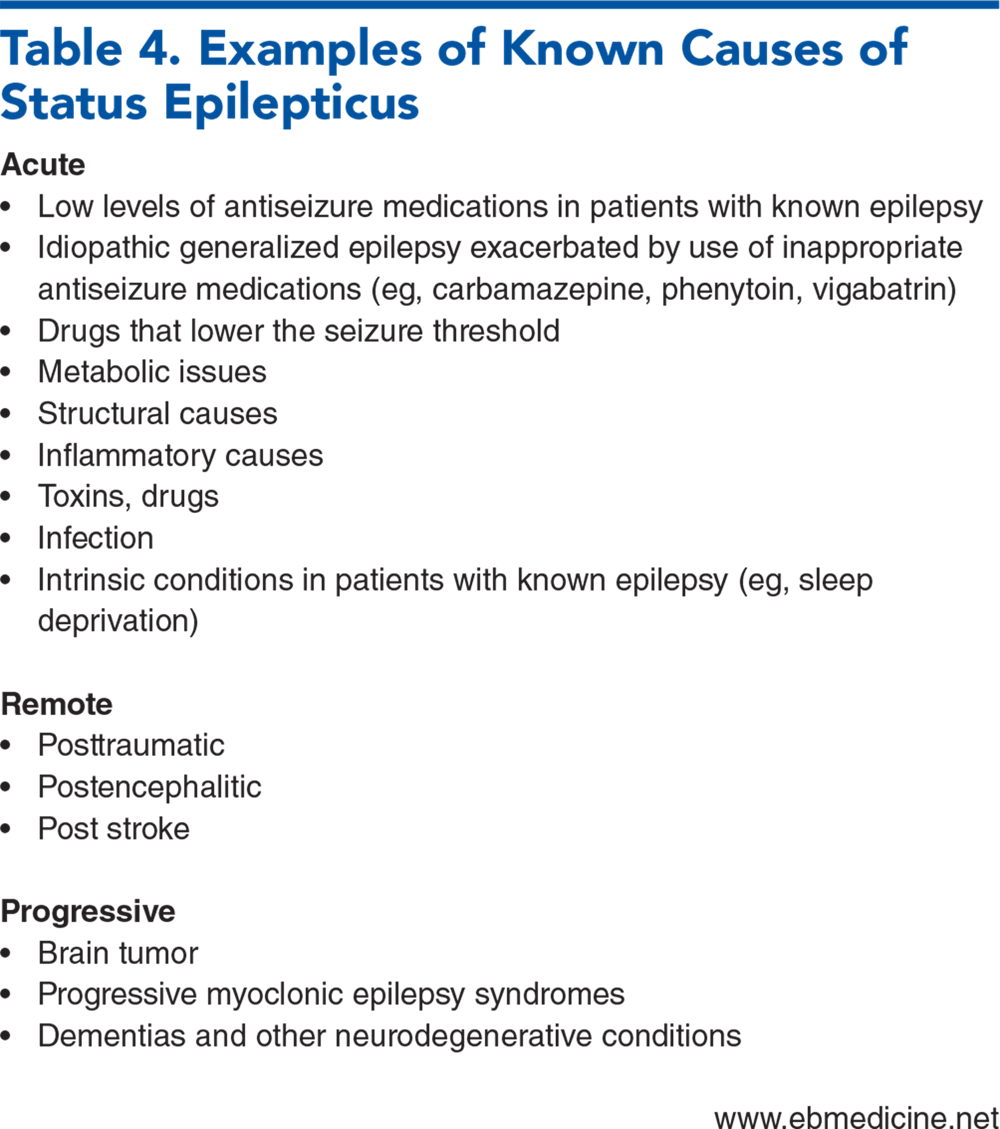
Subscribe for full access to all Tables.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
1. * Trinka E, Cock H, Hesdorffer D, et al. A definition and classification of status epilepticus—report of the ILAE Task Force on Classification of Status Epilepticus. Epilepsia. 2015;56(10):1515-1523. (Consensus statement) DOI: 10.1111/epi.13121
2. * Brophy GM, Bell R, Claassen J, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. 2012;17(1):3-23. (Guideline) DOI: 10.1007/s12028-012-9695-z
3. * Glauser T, Shinnar S, Gloss D, et al. Evidence-based guideline: treatment of convulsive status epilepticus in children and adults: report of the Guideline Committee of the American Epilepsy Society. Epilepsy Curr. 2016;16(1):48-61. (Guideline) DOI: 10.5698/1535-7597-16.1.48
40. * Alldredge BK, Gelb AM, Isaacs SM, et al. A comparison of lorazepam, diazepam, and placebo for the treatment of out-of-hospital status epilepticus. N Engl J Med. 2001;345(9):631-637. (Randomized controlled trial; 205 patients) DOI: 10.1056/NEJMoa002141
45. * Kapur J, Elm J, Chamberlain JM, et al. Randomized trial of three anticonvulsant medications for status epilepticus. N Engl J Med. 2019;381(22):2103-2113. (Randomized controlled trial; 384 patients) DOI: 10.1056/NEJMoa1905795
50. * Kanner AM, Bicchi MM. Antiseizure medications for adults with epilepsy: a review. JAMA. 2022;327(13):1269-1281. (Review) DOI: 10.1001/jama.2022.3880
54. * Shin J-W. Management strategies for refractory status epilepticus. Journal of Neurocritcal Care. 2023;16(2):59-68. (Review) DOI: 10.18700/jnc.230037
Subscribe to get the full list of 75 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: seizure, epilepsy, nonconvulsive, convulsive, electroencephalogram, myoclonic, tonic, benzodiazepine, midazolam, lorazepam, refractory, psychogenic
Destiny Marquez, MD; Rmneek Kaur, DO; Cappi Lay, MD
David M. Gillis, DO; Shana E. N. Ross, DO, MSc, FAAEM, FACEP
September 1, 2025
September 1, 2028 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933