Table of Contents
About This Issue
Fever in the returning international traveler presents a significant diagnostic challenge in the emergency department, where clinicians must rapidly evaluate a broad differential that includes both cosmopolitan infections and potentially life-threatening tropical diseases. Timely recognition and targeted management are required to reduce morbidity, mortality, and the risk of disease spread. This issue presents a structured, systematic approach to evaluating fever in recently returned travelers, with evidence-based recommendations for diagnosis and treatment of the 4 key infections most likely to cause serious illness: malaria, dengue, enteric fever, and leptospirosis. In this issue, you will learn:
Why travel history is the most critical component of the workup
How to recognize the clinical presentations of malaria, dengue, enteric fever, and leptospirosis, including key examination findings and overlapping features
How to select and interpret diagnostic tests for each infection based on timing of illness and available resources
Evidence-based treatment recommendations for malaria, including how disease severity guides management
How to manage dengue and recognize dengue warning signs
How antimicrobial resistance patterns should guide empiric antibiotic selection for enteric fever
When to initiate empiric treatment for leptospirosis
- About This Issue
- Abstract
- Case Presentations
- Introduction
- Critical Appraisal of the Literature
- Epidemiology, Etiology, and Pathophysiology
- Malaria
- Dengue
- Enteric Fever
- Leptospirosis
- Differential Diagnosis
- Prehospital Care
- Emergency Department Evaluation
- History
- Malaria
- Dengue
- Enteric Fever
- Leptospirosis
- Physical Examination
- Malaria
- Dengue
- Enteric Fever
- Leptospirosis
- Diagnostic Studies
- Malaria
- Dengue
- Enteric Fever
- Leptospirosis
- Treatment
- Malaria
- Dengue
- Enteric Fever
- Leptospirosis
- Special Populations
- Pregnant Patients
- Malaria
- Dengue
- Enteric Fever
- Leptospirosis
- Pediatric Patients
- Malaria
- Dengue
- Enteric Fever
- Leptospirosis
- Disposition
- Malaria
- Dengue
- Enteric Fever
- Leptospirosis
- Controversies and Cutting Edge
- Malaria
- Dengue
- Enteric Fever
- Leptospirosis
- Multiplex Polymerase Chain Reaction Assays
- Summary
- 5 Things That Will Change Your Practice
- Risk Management Pitfalls in the Emergency Department Evaluation and Management of Fever in Returning Travelers
- Time- and-Cost Effective Strategies
- Case Conclusions
- Clinical Pathways
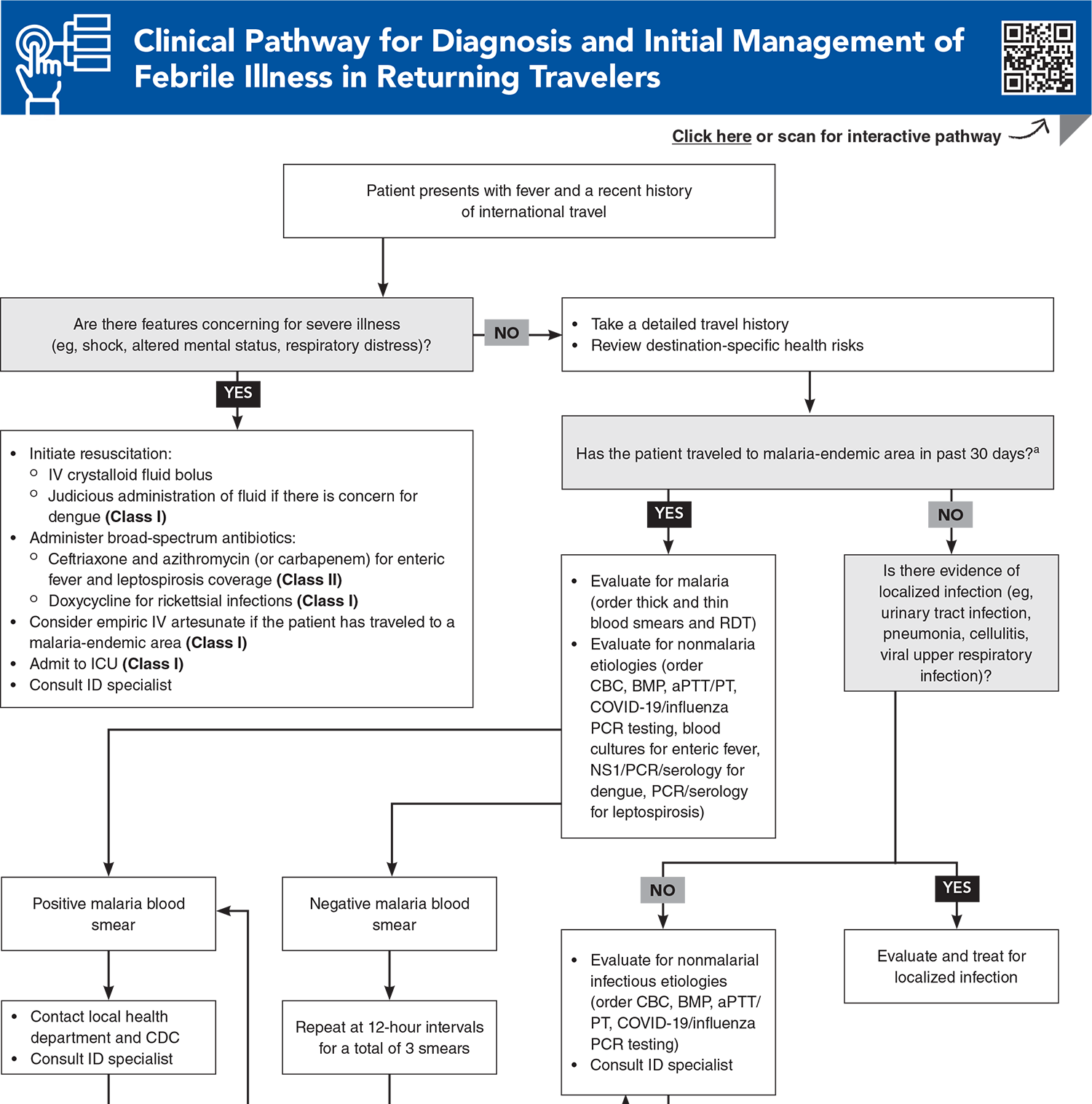
- Clinical Pathway for Diagnosis and Initial Management of Febrile Illness in Returning Travelers
- Clinical Pathway for Emergency Department Management of Malaria in Returning Travelers
- Clinical Pathway for Emergency Department Management of Suspected Dengue in Returning Travelers
- Clinical Pathway for Emergency Department Management of Suspected Enteric Fever in Returning Travelers
- Clinical Pathway for Emergency Department Management of Suspected Leptospirosis in Returning Travelers
- Tables and Figures
- References
Abstract
Fever in the returning international traveler presents a diagnostic challenge in the emergency department due to the wide range of potential infectious diseases that may be encountered abroad, many of which may manifest with nonspecific presentations. Malaria remains the most common and life-threatening tropical cause of fever and must be ruled out in all febrile patients returning from malaria-endemic regions. Other key infections to consider in returning travelers include dengue, enteric fever, and leptospirosis. Early recognition and treatment of these diseases can reduce morbidity and mortality and may help contain disease outbreaks. This review presents a structured, systematic approach to the timely evaluation of fever in returning international travelers, including evidence-based recommendations for the diagnosis and treatment of malaria, dengue, enteric fever, and leptospirosis.
Case Presentations
- She immigrated to the United States from Ghana as a child and recently traveled back there for her grandmother’s funeral, returning 3 days ago after a 2-week stay.
- Her vital signs are: temperature, 37.7°C; heart rate, 110 beats/min; blood pressure, 110/65 mm Hg; respiratory rate, 20 breaths/min; and oxygen saturation, 98% on room air. The physical examination is benign.
- Your initial impression is that she has an influenza-like illness. As you await the result of a rapid test for influenza and COVID-19, you try to recall other travel-related infections that you need to consider…
- She returned from the Dominican Republic 1 week ago.
- Her vital signs are: temperature, 38.2°C; heart rate, 120 beats/min; blood pressure, 100/78 mm Hg; respiratory rate, 22 breaths/min; and oxygen saturation, 100% on room air.
- On examination, her mucous membranes appear dry. She is tachycardic. Her lungs are clear. There is diffuse abdominal tenderness. You note a petechial rash on her arm distal to the blood pressure cuff.
- Based on her travel history and presentation, you suspect that your patient may have dengue, but you wonder which laboratory tests you should order…
- He recently returned from a 3-week trip to Pakistan, where he was visiting family and friends.
- His vital signs are: temperature, 38.9°C; heart rate, 52 beats/min; blood pressure, 130/70 mm Hg; respiratory rate, 22 breaths/min; and oxygen saturation, 98% on room air.
- On examination, his abdomen is diffusely tender and slightly distended with no peritoneal signs. There is a blanching maculopapular rash on his abdomen.
- The patient meets the criteria for systemic inflammatory response syndrome, so you order basic laboratory studies and blood cultures, and initiate resuscitation with IV crystalloid fluids. You consider which empiric antibiotics would be most appropriate for this patient…
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
Clinical Pathway for Managing Patients Presenting with Acute Diarrhea in Urgent Care
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Tables and Figures
Subscribe for full access to all Tables and Figures.
Buy this issue and
CME test to get 4 CME credits.
Key References
Following are the most informative references cited in this paper, as determined by the authors.
1. * Jensenius M, Han PV, Schlagenhauf P, et al. Acute and potentially life-threatening tropical diseases in Western travelers--a GeoSentinel multicenter study, 1996-2011. Am J Trop Med Hyg. 2013;88(2):397-404. (Multicenter retrospective observational study; 82,825 patients) DOI: 10.4269/ajtmh.12-0551
6. * Bottieau E, Clerinx J, Van den Enden E, et al. Fever after a stay in the tropics: diagnostic predictors of the leading tropical conditions. Medicine (Baltimore). 2007;86(1):18-25. (Prospective observational; 1962 patients) DOI: 10.1097/MD.0b013e3180305c48
17. * Yacoub S, Wills B. Dengue: an update for clinicians working in non-endemic areas. Clin Med (Lond). 2015;15(1):82-85. (Review) DOI: 10.7861/clinmedicine.15-1-82
30. * Parry CM, Hien TT, Dougan G, et al. Typhoid fever. N Engl J Med. 2002;347(22):1770-1782. (Review) DOI: 10.1056/NEJMra020201
36. * Rajapakse S, Fernando N, Dreyfus A, et al. Leptospirosis. Nat Rev Dis Primers. 2025;11(1):32. (Primer) DOI: 10.1038/s41572-025-00614-5
55. * Askling HH, Bruneel F, Burchard G, et al. Management of imported malaria in Europe. Malar J. 2012;11:328. (Position paper) DOI: 10.1186/1475-2875-11-328
99. * Cheng MP, Yansouni CP. Management of severe malaria in the intensive care unit. Crit Care Clin. 2013;29(4):865-885. (Review)DOI: 10.1016/j.ccc.2013.06.008
Subscribe to get the full list of 135 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: fever in travelers, febrile traveler, returning traveler, travel-related illness, travel medicine, tropical infections, tropical infectious disease, malaria, falciparum malaria, dengue, dengue warning signs, enteric fever, typhoid fever, paratyphoid fever, leptospirosis, antimalarial










 678-366-7933
678-366-7933