

|
|
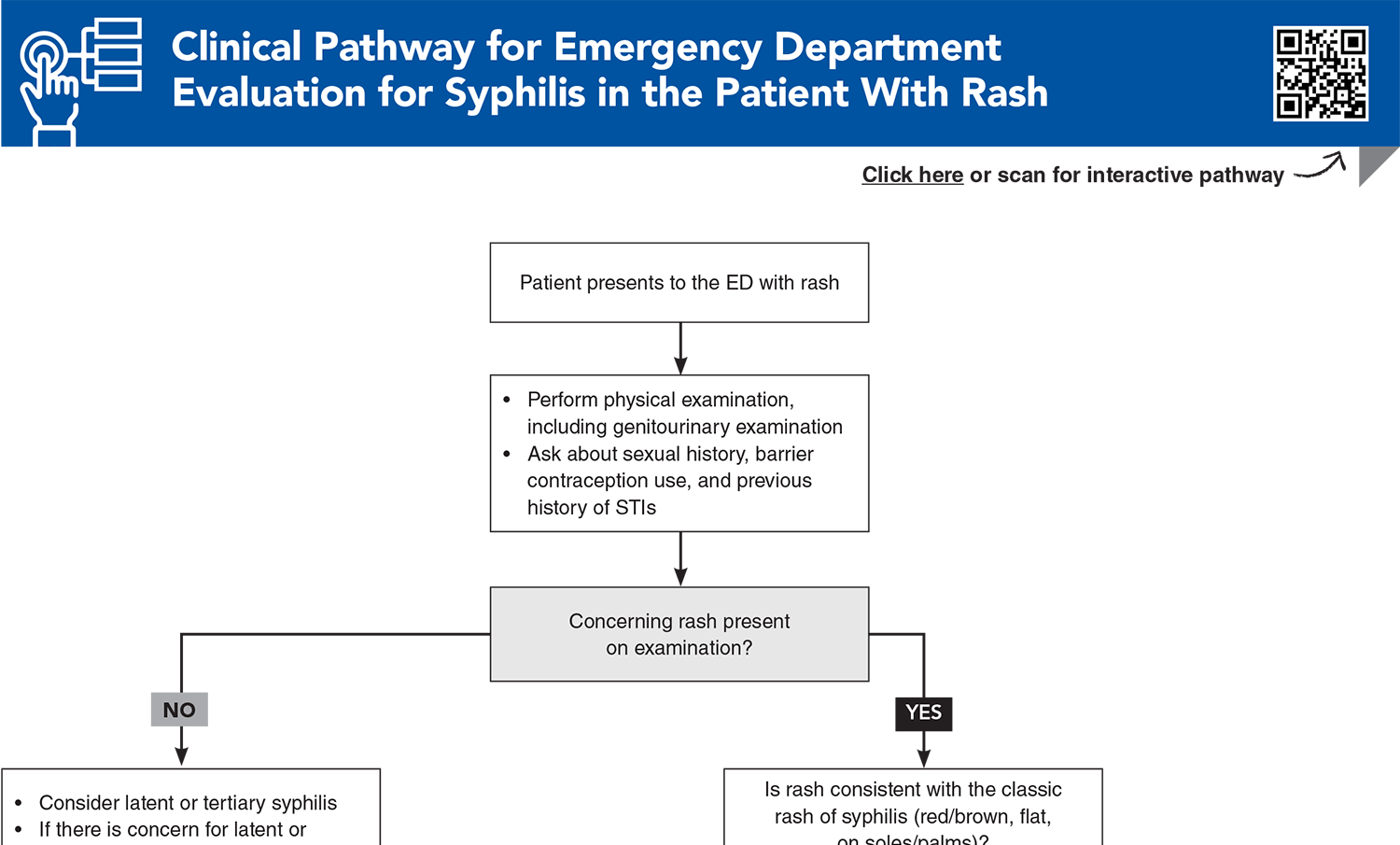
Syphilis is a sexually transmitted infection known as the “great imitator” due to its large variety of presentations, depending on the stage of the disease. Because of its prevalence and the possibility of severe outcomes, emergency clinicians must remain vigilant when evaluating patients, especially those in high-risk groups. Clinicians should be familiar with the treatment recommendations for the various stages of syphilis, including alternative regimens, when national drug shortages limit the availability of first-line treatments. This review discusses the various presentations, diagnostic options, and potential complications for syphilis, as well as current and emerging treatment recommendations.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
1. * New York City Department of Health and Mental Hygiene. The diagnosis, management, and prevention of syphilis: an update and review. 2019. Accessed December 10, 2025. (Review)
3. * Eppes CS, Stafford I, Rac M. Syphilis in pregnancy: an ongoing public health threat. Am J Obstet Gynecol. 2022;227(6):822-838. (Review) DOI: 10.1016/j.ajog.2022.07.041
5. * Hazra A, Collison MW, Davis AM. CDC sexually transmitted infections treatment guidelines, 2021. JAMA. 2022;327(9):870-871. (Guidelines) DOI: 10.1001/jama.2022.1246
9. * Ren M, Dashwood T, Walmsley S. The intersection of HIV and syphilis: update on the key considerations in testing and management. Curr HIV/AIDS Rep. 2021;18(4):280-288. (Review) DOI: 10.1007/s11904-021-00564-z
19. * Thean L, Moore A, Nourse C. New trends in congenital syphilis: epidemiology, testing in pregnancy, and management. Curr Opin Infect Dis. 2022;35(5):452-460. (Review) DOI: 10.1097/QCO.0000000000000875
22. * Wan Z, Zhang H, Xu H, et al. Maternal syphilis treatment and pregnancy outcomes: a retrospective study in Jiangxi Province, China. BMC Pregnancy Childbirth. 2020;20(1):648. (Analysis of Chinese database; 4210 women) DOI: 10.1186/s12884-020-03314-y
24. * Guidance for STD clinical preventive services for persons infected with HIV. Sex Transm Dis. 2001;28(8):460-463. (Committee recommendations) DOI: 10.1097/00007435-200108000-00007
30. * Clement ME, Okeke NL, Hicks CB. Treatment of syphilis: a systematic review. JAMA. 2014;312(18):1905-1917. (Systematic review; 102 articles) DOI: 10.1001/jama.2014.13259
Subscribe to get the full list of 43 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: STI, RPR, VDRL, neurosyphilis, congenital, primary, secondary, tertiary, latent, chancre, rash, treponemal, nontreponemal, penicillin, benzathine, benzylpenicillin, PrEP, HIV
Hilary H. Beason, MD, FACEP; Chen He, MD
Erik Blutinger, MD, MSc, FACEP; Daniel J. Egan, MD, MBA
January 1, 2026
January 1, 2029 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits. Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 4 Infectious Disease CME credits and 3 Pharmacology CME credits, subject to your state and institutional approval.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933


