

|
|
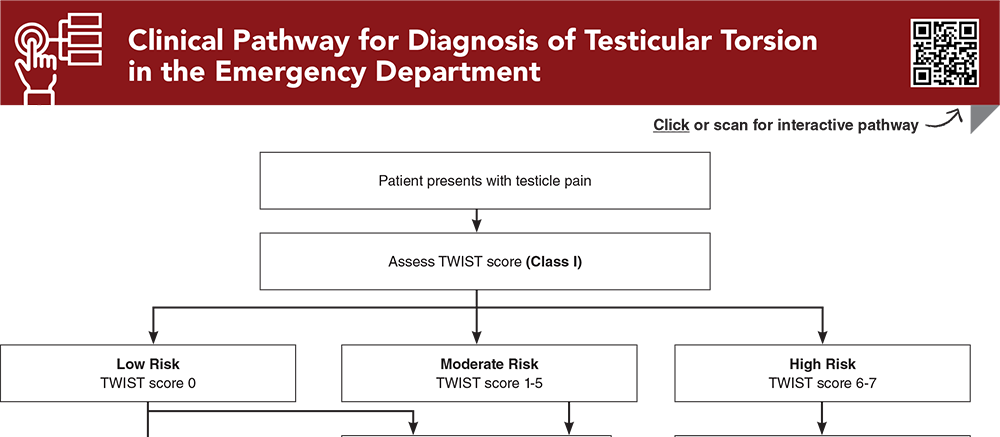
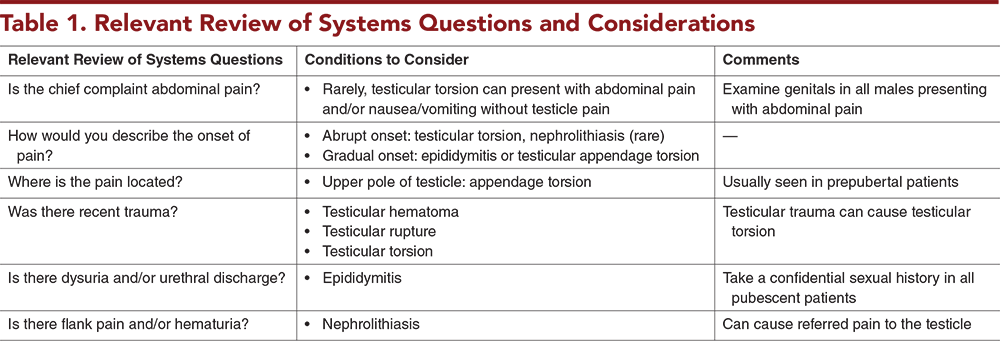
Testicular torsion is a urologic emergency, accounting for up to 15% of cases of acute scrotal pain. Rapid recognition and management are essential to ensure viability of the testis. Doppler ultrasound can be used to confirm the diagnosis of testicular torsion; however, recent studies suggest that a more judicious use of ultrasound may be safe, decrease delays in surgical management, and avoid unnecessary utilization of resources. This issue reviews the epidemiology and historical and physical examination findings of testicular torsion and other common causes of acute scrotal pain. The existing literature is reviewed and recommendations are provided to guide the emergency clinician in appropriate management and disposition of boys with acute scrotal pain.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
6. * Mori T, Ihara T, Nomura O. Diagnostic accuracy of point-of-care ultrasound for paediatric testicular torsion: a systematic review and meta-analysis. Emerg Med J. 2023;40(2):140-146. (Systematic review and meta-analysis; 4 studies, 784 patients) DOI: 10.1136/emermed-2021-212281
12. * Dias Filho AC, Oliveira Rodrigues R, Riccetto CL, et al. Improving organ salvage in testicular torsion: comparative study of patients undergoing vs not undergoing preoperative manual detorsion. J Urol. 2017;197(3 Pt 1):811-817. (Retrospective; 133 patients) DOI: 10.1016/j.juro.2016.09.087
26. * Gielchinsky I, Suraqui E, Hidas G, et al. Pregnancy rates after testicular torsion. J Urol. 2016;196(3):852-855. (Retrospective observational; 63 patients) DOI: 10.1016/j.juro.2016.04.066
29. * Santillanes G, Gausche-Hill M, Lewis RJ. Are antibiotics necessary for pediatric epididymitis? Pediatr Emerg Care. 2011;27(3):174-178. (Retrospective; 160 patients) DOI: 10.1097/PEC.0b013e31820d647a
37. * Sheth KR, Keays M, Grimsby GM, et al. Diagnosing testicular torsion before urological consultation and imaging: validation of the TWIST score. J Urol. 2016;195(6):1870-1876. (Prospective validation; 128 patients) DOI: 10.1016/j.juro.2016.01.101
45. * Frohlich LC, Paydar-Darian N, Cilento BG Jr, et al. Prospective validation of clinical score for males presenting with an acute scrotum. Acad Emerg Med. 2017;24(12):1474-1482. (Prospective cohort; 258 patients) DOI: 10.1111/acem.13295
46. * Barbosa JA, Tiseo BC, Barayan GA, et al. Development and initial validation of a scoring system to diagnose testicular torsion in children. J Urol. 2013;189(5):1859-1864. (Prospective, 338 patients; with retrospective validation, 220 patients) DOI: 10.1016/j.juro.2012.10.056
47. * Qin KR, Qu LG. Diagnosing with a TWIST: systematic review and meta-analysis of a testicular torsion risk score. J Urol. 2022;208(1):62-70. (Systematic review and meta-analysis; 13 studies, 1060 patients) DOI: 10.1097/JU.0000000000002496
56. * Friedman N, Pancer Z, Savic R, et al. Accuracy of point-of-care ultrasound by pediatric emergency physicians for testicular torsion. J Pediatr Urol. 2019;15(6):608.E1-608.E6. (Retrospective; 120 patients) DOI: 10.1016/j.jpurol.2019.07.003
58. * Demirbas A, Demir DO, Ersoy E, et al. Should manual detorsion be a routine part of treatment in testicular torsion? BMC Urol. 2017;17(1):84. (Retrospective; 57 patients) DOI: 10.1186/s12894-017-0276-5
Subscribe to get the full list of 68 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: acute scrotal pain, testicular torsion, groin pain, testicle pain, acute scrotum, testicular ischemia, cremasteric reflex, sequelae of testicular torsion, testicular appendage torsion, intravaginal torsion, extravaginal torsion, bell clapper deformity, acute epididymitis, inguinal hernia, varicoceles, hydroceles, TWIST score, whirlpool sign, manual testicular detorsion, open-book method, trans-scrotal near-infrared spectroscopy, NIRS
Mukuka Kangwa, MD; Yi Li, MD; Natasha A. Tejwani, MD; Hillary L. Copp, MD, MS; James Naprawa, MD
Kathleen Berg, MD, FAAEM, FACEP; Isaac Gordon, MD, FAAP
October 1, 2024
October 1, 2027 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAP Prescribed Credits, 4 AOA Category 2-B Credits.
Pediatric Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Pediatric Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933