Table of Contents
About This Issue
Urinary tract infection (UTI) is a common pathology of infancy, childhood, and adolescence, and is often diagnosed in pediatric patients in the emergency department (ED). Clinicians treating pediatric patients in the ED must be able to determine which patients warrant testing for a UTI, how to interpret results of diagnostic tests, and when to initiate empiric treatment. This issue reviews best practices for the diagnosis and management of UTI in pediatric patients presenting to the ED. In this issue, you will learn:
Common pathogens that cause urinary tract infections in pediatric patients
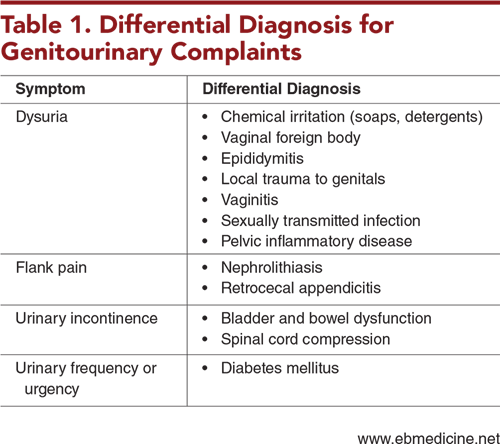
Conditions in the differential diagnosis of genitourinary complaints
Risk factors for UTI that can inform the decision of whether to obtain testing
General recommendations for obtaining diagnostic studies, as well as specific recommendations regarding urine collection, urinalysis, urine culture, blood cultures, and cerebrospinal fluid testing
Criteria to help make the decision of whether or not to treat the patient
Treatment recommendations including the route and duration of administration
Which patients should be admitted, which can be discharged safely, and which need follow-up imaging
-
About This Issue
-
Abstract
-
Case Presentations
-
Introduction
-
Critical Appraisal of the Literature
-
Etiology and Pathophysiology
-
Differential Diagnosis
-
Prehospital Care
-
Emergency Department Evaluation
-
History
-
Infants Aged <2 Months
-
Children Aged 2 Months to 2 Years
-
Children Aged >2 Years
-
Adolescents
-
Children of All Ages
-
Urinary Tract Infection Prevalence in Viral Illness
-
Physical Examination
-
Diagnostic Studies
-
General Recommendations
-
Urinalysis
-
Catheterization and Suprapubic Aspiration
-
Urine Bag
-
Other Methods of Urine Collection
-
Urine Culture
-
Blood Cultures
-
Cerebrospinal Fluid Testing
-
Decision to Treat
-
Using Urinalysis Results for Treatment Decisions
-
Using Urine Culture Results for Treatment Decisions
-
Additional Considerations for Treatment Decisions
-
Asymptomatic Bacteriuria
-
Sterile Pyuria
-
Summary of Considerations for Treatment
-
Treatment
-
Initiation of Antibiotics
-
Route of Antibiotic Administration
-
Treatment of Lower Urinary Tract Infection
-
Treatment of Pyelonephritis
-
Treatment of Infants
-
Resistant Organisms
-
Antibiotic Therapy Duration
-
Special Populations
-
Children With Urinary Tract Anomalies
-
Children With Neurogenic Bladder
-
Children Who Have Recently Received Antibiotics
-
Concern for Urosepsis
-
Controversies and Cutting-Edge
-
Controversies
-
Utility of Renal Bladder Ultrasound
-
Antibiotic Prophylaxis for Patients With Known Vesicoureteral Reflux
-
Cutting-Edge Research
-
Biomarkers
-
Contrast-Enhanced Ultrasound
-
Disposition
-
Follow-up Imaging
-
Summary
-
Time- and Cost-Effective Strategies
-
5 Things That Will Change Your Practice
-
Risk Management Pitfalls in Children With Suspected Urinary Tract Infection
-
Case Conclusions
-
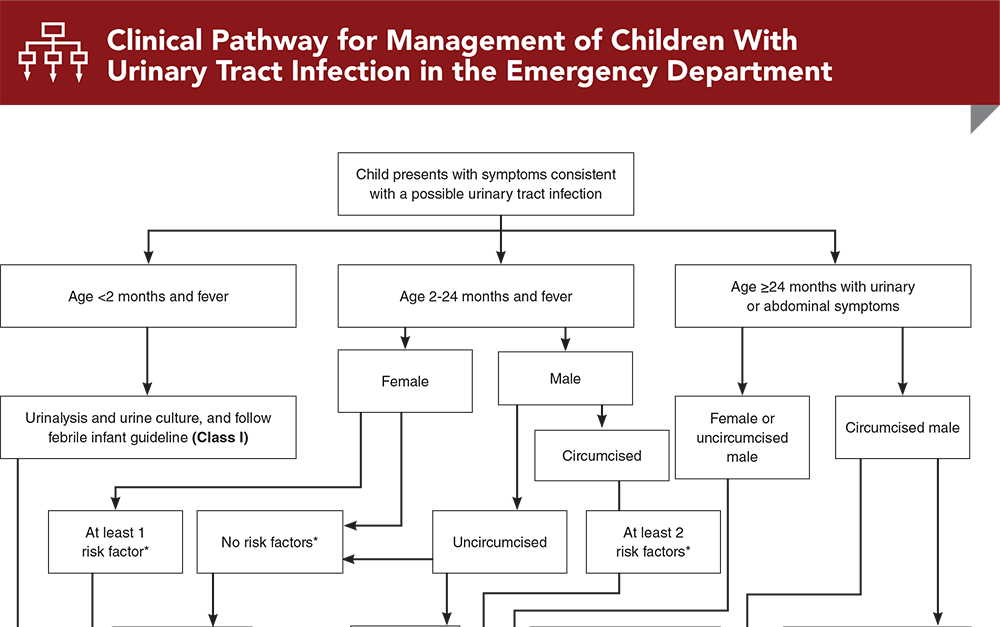
Clinical Pathway for Management of Children With Urinary Tract Infection in the Emergency Department
-
Tables and Figures
-
References
Abstract
Urinary tract infection (UTI) is a common diagnosis in pediatric patients presenting to the emergency department. Although there are several evidence-based guidelines for UTI, they have small variations that can make the workup and management for UTI challenging. This issue reviews the current state of the literature and best practices for the diagnosis and management of UTI in children presenting to the emergency department, including criteria to help the clinician decide whether to test a patient’s urine, the best method for urine testing based on the clinical scenario, and how to manage the patient based on the results of urine testing. Also discussed is the best antibiotic choice for specific patients, including the route of administration and duration.
Case Presentations
-
The girl has no past medical history and a normal birth history. Her parents say that she felt warm to the touch earlier today, so they took a rectal temperature, which was 100.8°F (38.2°C). They called their pediatrician’s office and were told to take the child to the ED. The parents tell you the girl has otherwise been asymptomatic, has continued to take her regular feeds, and has normal urine output.
-
On physical examination, the girl is well-appearing, with no focal signs of infection. You initiate a standard workup for a febrile infant. Her CBC, CRP, and procalcitonin are within normal limits, and a blood culture is sent. You obtain urine for a urinalysis via sterile catheterization of the urethra. The urinalysis shows 3+ leukocyte esterase and many bacteria, with no nitrites. You send the urine for culture as well. The girl continues to be well-appearing.
-
How do you interpret her urinalysis? What further management should you provide?
-
The parents tell you he had a maximum temperature of 100.6°F (38.1°C). Prior to the onset of his fever, he had a few days of cough and rhinorrhea, which have now resolved.
-
You note a well-appearing child who is uncircumcised and has a normal physical examination.
-
Should you work up this child for a possible urinary tract infection? If so, how should you obtain a urine specimen? What are the diagnostic criteria for treatment? How would you treat him if you determine that he has a urinary tract infection?
-
The girl has no significant past medical history. She has been afebrile and denies abdominal pain or any changes to her vaginal discharge. She reports that she has had 2 lifetime sexual partners. She states that she has never been tested for a sexually transmitted infection, as she does not think it has been necessary, since she is in a monogamous relationship.
-
What is your differential diagnosis for this patient? What should your evaluation of this patient include?
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
Clinical Pathway for Management of Children With Urinary Tract Infection in the Emergency Department
Subscribe to access the complete flowchart to guide your clinical decision making.
Tables and Figures
Subscribe for full access to all Tables and Figures.
Buy this issue and
CME test to get 4 CME credits.
Key References
Following are the most informative references cited in this paper, as determined by the authors.
3. * Shaikh N, Morone NE, Lopez J, et al. Does this child have a urinary tract infection? JAMA. 2007;298(24):2895-2904. (Systematic review; 12 studies; 8837 patients) DOI: 10.1001/jama.298.24.2895
8. * Mattoo TK, Shaikh N, Nelson CP. Contemporary management of urinary tract infection in children. Pediatrics. 2021;147(2):e2020012138. (Review) DOI: 10.1542/peds.2020-012138
12. * Roberts KB, Subcommittee on Urinary Tract Infection, Steering Committee on Quality Improvement Management. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics. 2011;128(3):595-610. (Clinical practice guideline) DOI: 10.1542/peds.2011-1330
19. * Shaikh N, Hoberman A, Hum SW, et al. Development and validation of a calculator for estimating the probability of urinary tract infection in young febrile children. JAMA Pediatr. 2018;172(6):550. (Case control study; 2070 patients) DOI: 10.1001/jamapediatrics.2018.0217
86. Peters CA, Skoog SJ, Arant BS Jr, et al. Management and screening of primary vesicoureteral reflux in children. 2017. Accessed December 1, 2023. (Guidelines)
Subscribe to get the full list of 96 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: urinary tract infection, UTI, pyelonephritis, bacteremia, meningitis, circumcision, renal scarring, UTI prevention, renal bladder ultrasound, cystitis, urine collection methods, catheterization, suprapubic aspiration, urine bag, quick-wee method, urine culture, uropathogen, urinalysis, rapid urinalysis, sterile pyuria, asymptomatic bacteriuria, neurogenic bladder, urosepsis, vesicoureteral reflux









 678-366-7933
678-366-7933