

|
|
This content was adapted from: Edlow JA. The timing-and-triggers approach to the patient with acute dizziness. Emerg Med Pract. 2019;21(12):1-24. Used with permission of EB Medicine.
Acute dizziness is a common presentation in the urgent care setting. Due to newer research, the diagnostic approach to dizziness has changed, now focusing on its timing and triggers of instead of the patient’s symptom quality (vertigo vs lightheadedness). Each timing-and-triggers category has its own differential diagnosis and diagnostic approach, which will aid clinicians in distinguishing benign causes of dizziness from life-threatening causes. Brain imaging, even with magnetic resonance imaging, has important limitations in ruling out stroke presenting with dizziness, elevating accurate clinical diagnosis to an even greater level of importance. Benign paroxysmal positional vertigo can be treated with repositioning maneuvers at the bedside, offering cost-effective management options.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
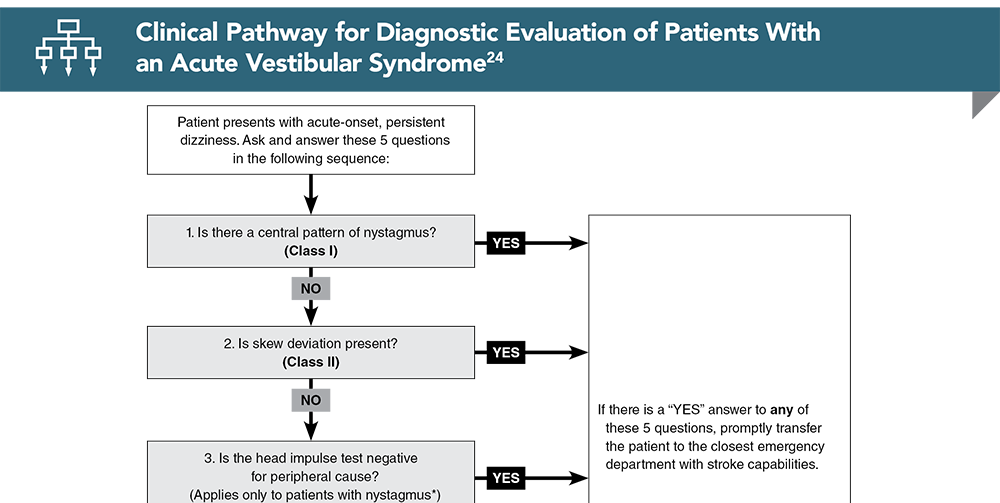
Subscribe to access the complete flowchart to guide your clinical decision making.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
8. * Edlow JA, Carpenter C, Akhter M et al. Guidelines for reasonable and appropriate care in the emergency department 3 (GRACE-3): acute dizziness and vertigo in the emergency department. Acad Emerg Med. 2023;30(5):442-486. DOI: 10.1111/acem.14728
24. * Edlow JA. Diagnosing patients with acute-onset persistent dizziness. Ann Emerg Med. 2018;71(5):625-631. (Review article) DOI: 10.1016/j.annemergmed.2017.10.012
29. * Paul NL, Simoni M, Rothwell PM, et al. Transient isolated brainstem symptoms preceding posterior circulation stroke: a population-based study. Lancet Neurol. 2013;12(1):65-71. (Prospective population-based study; 1141 stroke patients) DOI: 10.1016/S1474-4422(12)70299-5
37. * Atzema CL, Grewal K, Lu H, et al. Outcomes among patients discharged from the emergency department with a diagnosis of peripheral vertigo. Ann Neurol. 2015;79(1):32-41. (Retrospective population-based cohort; 41,794 discharged ED dizzy patients) DOI: 10.1002/ana.24521
43. * Arch AE, Weisman DC, Coca S, et al. Missed ischemic stroke diagnosis in the emergency department by emergency medicine and neurology services. Stroke. 2016;47(3):668-673. (Retrospective cohort study; 485 patients) DOI: 10.1161/STROKEAHA.115.010613
49. * Kerber KA, Morgenstern LB, Meurer WJ, et al. Nystagmus assessments documented by emergency physicians in acute dizziness presentations: a target for decision support? Acad Emerg Med. 2011;18(6):619-626. (Chart review; 1091 patients) DOI: 10.1111/j.1553-2712.2011.01093.x
50. * Grewal K, Austin PC, Kapral MK, et al. Missed strokes using computed tomography imaging in patients with vertigo: population-based cohort study. Stroke. 2015;46(1):108-113. (Retrospective cohort study; 41,794 patients) DOI: 10.1161/STROKEAHA.114.007087
Subscribe to get the full list of 90 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: dizzy, dizziness, lightheaded, vertigo, BPPV, vestibular syndrome, benign paroxysmal positional vertigo, head impulse test, HIT, HINTS, ATTEST, GRACE-3, CPPV, nystagmus, posterior circulation, skew, saccade, gait, migraine, Dix-Hallpike, Epley, Semont, Lempert
Joseph Toscano, MD, FCUCM
Sean M. McNeeley, MD, FCUCM
February 1, 2024
February 1, 2027 CME Information
4 AMA PRA Category 1 Credits™. 4 AOA Category 2-B Credits. 4 AAFP Prescribed Credits Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 1 Stroke CME credit.
Evidence-Based Urgent Care • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Evidence-Based Urgent Care issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933