Table of Contents
-
Abstract
-
Clinical Guidelines
-
The Red Eye
-
History
-
The Physical Examination
-
Visual Acuity
-
The External Eye Examination
-
The Pupil
-
The Slit Lamp
-
Topical Anesthetics
-
Eyelid Eversion
-
Tonometry
-
Fluorescein Staining
-
Funduscopy
-
Common, Benign Causes Of A Red Eye
-
Bacterial Conjunctivitis
-
Gonococcal Conjunctivitis
-
Chlamydial Conjunctivitis
-
Viral Conjunctivitis
-
Allergic Conjunctivitis
-
Blepharitis
-
Pinguecula And Pterygium
-
Corneal Abrasions
-
Superficial Keratitis
-
Less Common (But More Serious) Causes Of The Red Eye
-
Corneal Ulcers
-
Acute Anterior Uveitis
-
HSV Keratitis
-
Herpes Zoster
-
Fungal Conjunctivitis
-
Acute Angle-Closure Glaucoma
-
Scleritis
-
Episcleritis
-
The Red Eye (continued)
-
Less Common (But More Serious) Causes Of The Red Eye
-
Corneal Ulcers
-
Acute Anterior Uveitis
-
HSV Keratitis
-
Herpes Zoster
-
Fungal Conjunctivitis
-
Acute Angle-Closure Glaucoma
-
Scleritis
-
Episcleritis
-
Corneal Perforation
-
Endophthalmitis
-
Pediatric Considerations
-
Bacterial Conjunctivitis
-
Viral Conjunctivitis
-
Neonatal Conjunctivitis
-
Kawasaki Disease
-
Conclusion
-
The Swollen Eye
-
Bacterial Infections
-
Fungal Infections
-
Inflammatory Conditions
-
Tumors
-
Pediatric Considerations
-
Periorbital Cellulitis/Orbital Cellulitis
-
Dacryocystitis
-
Tumors
-
Conclusion
-
Acute Vision Loss
-
History
-
Physical Examination
-
Retinal Detachment
-
Double Vision
-
Acute Vision Loss Under The Age Of 50
-
Other Causes
-
Vision Loss Over The Age Of 60
-
Central Retinal Artery Occlusion
-
Central Retinal Vein Occlusion
-
Temporal Arteritis
-
Infants
-
Children
-
Adolescents
-
Conclusion
-
General Conclusion
-
Risk Management
-
Cost-Effective Strategies For Patients With Eye Disorders
-
Clinical Pathway: Management Of The Red Eye
-
Clinical Pathway: Management Of The Red Eye (continued)
-
Clinical Pathway: Diagnosing The Swollen EYE In Adults
-
Clinical Pathway: Diagnosing Acute Vision Loss In Adults
-
Tables and Figures
-
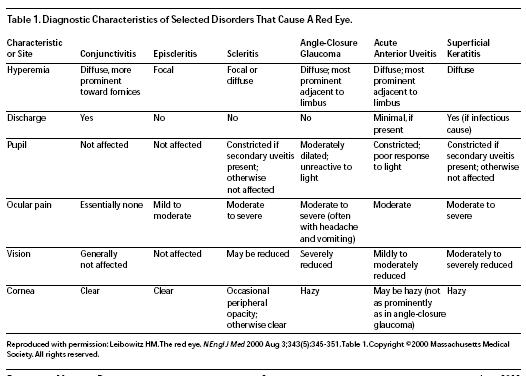
Diagnostic Characteristics of Selected Disorders That Cause A Red Eye
-
Glossary Of Terms
-
Treatment Of Acute Angle Closure Glaucoma
-
Therapy For Neonatal Conjunctivitis
-
Key Points In Managing The Red Eye
-
HSV dendrites
-
Sagittal section of orbit
-
Nasolacrimal apparatus
-
References
Abstract
EYE problems are common in every ED. While the exact number of emergency visits for eye complaints remains unknown, in the year 2000, nearly 4 million patients presented to U.S. EDs with a complaint referable to the ear or eye.1 The American Academy of Ophthalmology (AAO) estimates that one-third of all Americans have some ocular abnormality. Of these, one-quarter need corrective refraction to achieve normal vision. In all, 3 million Americans have impaired vision despite correction, and 890,000 are legally blind.2
Clinical Guidelines
In the past several years, the AAO has published "Preferred Practice Patterns" on a variety of subjects. Each subcommittee of the AAO reviews the medical literature of the previous five years on a particular subject (e.g., conjunctivitis, blepharitis, acute angle-closure glaucoma, etc.). The Committee recommendations are rated A to C with respect to clinical importance, "A" being most important; "B," moderately important; and "C," relevant but not critical. The clinical evidence is also evaluated on a scale of I to III, with Level I reflecting at least one well-designed randomized clinical trial; Level II, non-randomized, case-controlled, or multiple-time trials; and Level III, case reports, descriptive studies, or expert opinion. These guidelines are discussed in further detail in the subsequent sections of this article.
"The eye is the jewel of the body."—Henry David Thoreau
(1817-1862), U.S. essayist, poet, naturalist3
The Red Eye
While the red eye is a very frequent complaint in the ED, there are no definite data on its overall prevalence.4 The most common causes of the red eye include viral, bacterial, and allergic conjunctivitis. While emergency physicians are capable of treating the majority of patients who complain of a red eye, it is important to differentiate benign and selflimited conditions from more serious processes. (See Table 1.) Such vision-threatening conditions include acute angleclosure glaucoma, scleritis, uveitis, and keratitis. (See Table 2.)
History
The AAO categorizes the following elements of the history as "A," or most important; however, the evidence for these is rated as Level III:
-
Symptoms and signs: itching, discharge, pain, photophobia, blurred vision,5 colored halos around lights, headache, or brow pain6
-
Duration of symptoms
-
Unilateral vs. bilateral
-
Character of the discharge: purulent vs. clear
-
Recent exposure to an infected individual
-
Trauma: mechanical (as in rubbing an irritated eye) or foreign body, chemical, ultraviolet (UV) light (welder's flash, excessive sunlight, skiing without sunglasses, tanning booth, etc.)
-
Contact lens wear: the type of lens, duration of wear, hygiene, etc.
-
Associated symptoms that may be related to systemic disease: genital discharge, dysuria, upper respiratory infection (URI), skin and mucosal lesions, joint swelling
-
Allergy: any systemic complaints
-
Use of topical (especially ophthalmic) and/or systemic medications
-
Previous episodes of conjunctivitis
-
Pregnancy status5
-
Family history of acute angle-closure glaucoma (this is given a rating of A-II)6 The following are considered moderately important, again with Level III evidence:
-
Use of personal care items (including eyeliners and other cosmetics)
-
Previous ophthalmic surgery
-
Presence of immune dysfunction (e.g., HIV, chemotherapy, immunosuppression)
-
Prior allergic phenomena, such as atopy or Stevens- Johnson syndrome
The social history is considered relevant but not critical, again with Level III evidence:
-
Alcohol and tobacco use
-
Occupation and hobbies (e.g., welding, skiing, gardening)
-
Travel
-
Sexual activity1
Other relevant questions may include exposure to metal hitting metal (hammering) or other foreign body exposure (drilling, grinding, etc.).
Risk Management
1. "An eye patch never hurt anyone."
Au contraire! The patient with a corneal ulcer who gets an eye patch is at risk for perforation. Do not patch corneal abrasions secondary to contact lens use.
2. "He just had some eye pain. That's not an indication for visual acuities."
Having an eye complaint (and some say having an eye) is an indication for visual acuities. They are the "vital sign" of the eye.
3. "I know he had a lot of pus leaking from the eye, but I thought he would do fine with some Sulamyd."
This gentleman had gonococcal ophthalmia and was admitted the next day. Clues to this diagnosis include copious pus; an angry, often-hemorrhagic sclera; preauricular adenopathy; and anterior chamber inflammation. Gram's stain of the discharge will reveal the gram-negative diplococci within the leukocytes. Such patients require admission and parenteral antibiotics.
4. "Since the H. flu vaccine, I've been sending all kids with periorbital cellulitis home on oral antibiotics."
This child did not do well, even after decompressive surgery to the orbit. While it is true that the fierceness of this disease has relented in the past decade, the decision to treat as an outpatient must be made on an individual basis. Children who appear toxic, those with proptosis or impairment of extraocular motions, and patients with decreased vision need admission and parenteral antibiotics.
5. "It looked like he had fire ant bites to his eyelids. Heck, they even bit him on the tip of his nose."
Hel-looo…fire ant bites!? Patients with herpes zoster need acyclovir, not Benadryl.
6. "We don't do fluorescein exams in our ED."
Start. Fluorescein exams are essential in diagnosing keratitis and corneal abrasions. They are also helpful in detecting corneal ulcers and corneal perforations.
7. "He was complaining of eye pain. I told him to take a few days off his job as a machinist and it would get better."
Intraocular foreign bodies rarely get better without surgery. A history of metal-on-metal exposure is key. Look for an irregular pupil. A Seidel test (see text) may be positive for leakage of aqueous humor.
8. "She was just another elderly woman with conjunctivitis who came to the ED in the middle of the night."
By the time the ophthalmologist saw her three days later, her IOP was over 80. Conjunctivitis usually does not present with severe eye pain, hazy cornea, and unreactive pupil. Check IOPs in suspicious cases; at the very least, compare the tension in each eye by fingertip assessment.
9. "I looked in his eye and didn't see a foreign body. All he had were a lot of vertical scratches to his cornea."
And a foreign body under the lid. Evert the lids when a patient complains of a foreign body sensation—especially when they demonstrate an "ice rink" sign.
10. "I thought she was malingering. She said she was almost blind in her right eye, but she blinked when I pretended to poke her in the eye. Besides, her pupil reacted to light."
She had optic neuritis, not hysteria. Patients with ON may still have a light reflex; the swinging flashlight test would have been abnormal (if it had been done). Blind patients still blink when a threat is made to their eye secondary to the corneal reflex in response to a rush of air. (Plus, there was nothing wrong with this lady's other eye.)
Tables and Figures
References
Evidence-based medicine requires a critical appraisal of the literature based upon study methodology and number of subjects. Not all references are equally robust. The findings of a large, prospective, randomized, and blinded trial should carry more weight than a case report.
To help the reader judge the strength of each reference, pertinent information about the study, such as the type of study and the number of patients in the study, will be included in bold type following the reference, where available. In addition, the most informative references cited in the paper, as determined by the authors, will be noted by an asterisk (*) next to the number of the reference.
-
McCaig LF, Ly N. National Hospital Ambulatory Medical Care Survey: 2000 Emergency Department Summary. Advance Data No. 326. April 22, 2002. Centers for Disease Control and Prevention. (U.S. government data)
-
* Comprehensive Adult Medical Eye Evaluation. Preferred Practice Pattern. American Academy of Ophthalmology 2000 Sept. (Clinical practice guideline)
-
As cited in: The Ultimate Success Quotations Library, 1997.
-
* Leibowitz HM. The red eye. N Engl Med 2000 Aug 3;343(5):345- 351. (Systematic review)
-
* Conjunctivitis. Preferred Practice Pattern. American Academy of Ophthalmology 1998 Sept. (Clinical practice guideline)
-
Primary Angle Closure. Preferred Practice Pattern. American Academy of Ophthalmology 2000 Sept. (Clinical practice guideline)
-
Powers DW, Meador SA. Testing visual acuity in the emergency department: a simple method of correcting refractive error by using the hand-held ophthalmoscope. Ann Emerg Med 1986 Jul;15(7):818-819. (Description of method)
-
Rose GE, Pearson RV. Unequal pupil size in patients with unilateral red eye. BMJ 1991 Mar 9;302(6776):571-572. (Consecutive series)
-
Au YK, Henkind P. Pain elicited by consensual pupillary reflex: a diagnostic test for acute iritis. Lancet 1981 Dec 5;2(8258):1254-1255. (Consecutive series)
-
* Talbot EM. A simple test to diagnose iritis. BMJ 1987 Oct 3;295(6602):812. (Consecutive series)
-
Roberts JR, Hedges JR, eds. Clinical Procedures in Emergency Medicine. Philadelphia; W.B. Saunders;1998. (Textbook)
-
Anderson DF, Sullivan PM, Luff AJ, et al. Direct ophthalmoscopy versus slit lamp biomicroscopy in diagnosis of the acute red eye. J R Soc Med 1998 Mar;91(3):127-128. (Prospective, controlled clinical trial; 98 patients)
-
Sklar DP, Lauth JE, Johnson DR. Topical anesthesia of the eye as a diagnostic test. Ann Emerg Med 1989 Nov;18(11):1209-1211. (Convenience sample; 71 patients)
-
Bartfield JM, Holmes TJ, Raccio-Robak N. A comparison of proparacaine and tetracaine eye anesthetics. Acad Emerg Med 1994 Jul;1(4):364-367. (Prospective, volunteer, randomized, controlled trial; 23 subjects)
-
Brady MD, Hustead RR, Robinson RH, et al. Dilution of proparacaine in balanced salt solution reduces pain of anesthetic instillation in the eye. Reg Anesth 1994 May;19(3):196-198. (Randomized, controlled trial; 42 adults)
-
Aylward GW, Wilson RS. Contamination of dropper bottles with tear fluid in an ophthalmic outpatient clinic. Br Med J (Clin Res Ed) 1987 Jun 20;294(6587):1587. (Descriptive)
-
Hoffman CJ, Laibson PR. Corneal manifestations of local and systemic therapy. In: Krachmer JH, Mannis MJ, Holland E, eds. Cornea. St. Louis: Mosby; 1997:1023-1028. (Textbook chapter)
-
Bode DD, Manson RA. An expedient lid retracter. J Pediatr Ophthalmol Strabismus 1978 Jan;15(1):54.
-
* Alward WLM. Medical management of glaucoma. N Engl Med 1998 Oct 29;339(18):1298-1307. (Review)
-
Hessemer V, Rossler R, Jacobi KW. Tono-pen, a new tonometer. Internat Ophthal 1989 Jan;13(1-2):51-56. (2 studies comparing the Tono-pen with the Goldmann tonometer)
-
Bafa M, Lambrinakis I, Dayan M, et al. Clinical comparison of the measurement of the IOP with the ocular blood flow tonometer, the Tono-pen XL and the Goldmann applanation tonometer. Acta phthalmol Scand 2001 Feb;79(1):15-18. (Randomized, controlled trial; 99 eyes)
-
agington J, Sutehall GM, Whipp P. Tonometer disinfection and viruses. Br J Ophthalmol 1983 Oct;67(10):674-676. (Microbiologic study)
-
Chung CW, Cohen EJ. Eye disorders: bacterial conjunctivitis. West J Med 2000 Sep;173(3):202-205. (Systematic review)
-
Sheikh A, Hurwitz B. Topical antibiotics for acute bacterial conjunctivitis: a systematic review. Br J Gen Pract 2001 Jun;51(467):473-477. (Systematic review of six published clinical trials)
-
Friedlaender MH. A review of the causes and treatment of bacterial and allergic conjunctivitis. Clin Ther 1995 Sep- Oct;17(5):800-810; discussion 779. (Review; 213 references)
-
* Sheik A, Hurwitz B, Cave J. Antibiotics versus placebo for acute bacterial conjunctivitis. Cochrane Eyes and Vision Group. Cochrane Database of Systematic Reviews. 2001; issue 4. (Systematic review)
-
Adler AG, McElwain GE, Merli GJ, et al. Systemic effects of eye drops. Arch Intern Med 1982 ec;142(13):2293-2294. (Review)
-
Kettenmeyer A, Jauch A. The French Lomefloxacin Group. A double-blind double-dummy multicenter equivalence study comparing topical Lomefloxacin 0.3% twice daily with Norfloxacin 0.3% four times daily in the treatment of acute bacterial conjunctivitis. J Drug Assess 1998;1(1):69-80. (Multicenter, double- blind clinical trial)
-
Friedlaender MH. Twice-a-day versus four-times-a-day ofloxacin treatment of external ocular infection. CLAO J 1998 Jan;24(1):48-51. (Prospective, randomized, controlled trial; 50 patients)
-
Soukiasian S, Baum J. Bacterial conjunctivitis. In: Krachmer JH, Mannis MJ, Holland E, eds. Cornea. St. Louis: Mosby; 1997:758- 772. (Textbook chapter)
-
Wan WL, Farkas GC, May WN, et al. The clinical characteristics and course of adult gonococcal conjunctivitis. Am J Ophthalmol 1986 Nov 15;102(5):575-583. (Retrospective; 21 cases)
-
Haimovici R, Roussel TJ. Treatment of gonococcal conjunctivitis with single-dose intramuscular ceftriaxone. Am J Ophthalmol 1989 May 15;107(5):511-514. (Consecutive series; 13 patients)
-
Viswalingam ND, Darougar S, Yearsley P. Oral doxycycline in the treatment of adult chlamydial ophthalmia. Br J Ophthalmol 1986 Apr;70(4):301-304. (Comparative; 93 patients)
-
Lindquist TD. Conjunctivitis: an overview and classification. In: Krachmer JH, Mannis MJ, Holland E, eds. Cornea. St. Louis: Mosby; 1997:745-757. (Textbook chapter)
-
Ward JB, Siojo LG, Waller SG. A prospective, masked clinical trial of trifluridine, dexamethasone, and artificial tears in the treatment of epidemic keratoconjunctivitis. Cornea 1993 May;12(3):216-221 (Prospective, randomized, controlled trial; 74 patients)
-
Shiuey Y, Ambati BK, Adamis AP. A randomized, double-masked trial of topical ketorolac versus artificial tears for treatment of viral conjunctivitis. Ophthalmology 2000 Aug;107(8):1512-1517. (Randomized, controlled trial; 117 patients)
-
Stamler JF. Viral conjunctivitis. In: Krachmer JH, Mannis MJ, Holland E, eds. Cornea. St. Louis: Mosby; 997;773-777. (Textbook chapter)
-
* Bielory L, Goodman PE, Fisher EM. Allergic ocular disease. A review of pathophysiology and clinical presentations. Clin Rev Allergy Immunol 2001 Apr;20(2):183-200. (Systematic review)
-
Raizman MB, Rothman JS, Maroun F, et al. Effect of eye rubbing on signs and symptoms of allergic conjunctivitis in cat-sensitive individuals. Ophthalmology 2000 Dec;107(12):2158-2161. (Two comparative, controlled clinical trials; 13 patients in the first and 20 patients in the second)
-
Lanier BQ, Tremblay N, Smith JP, et al. A double-masked comparison of ocular decongestants as therapy for allergic conjunctivitis. Ann Allergy 1983 Mar;50(3):174-177. (Prospective, randomized, double-blind trial; 89 patients)
-
Tauber J, Raizman MB, Ostrov CS, et al. A multicenter comparison of the ocular efficacy and safety of diclofenac 0.1% solution with that of ketorolac 0.5% solution in patients with acute easonal allergic conjunctivitis. J Ocul Pharmacol Ther 1998 Apr;14(2):137- 145. (Multicenter, prospective, randomized, controlled trial; 60 patients)
-
Laibovitz RA, Koester J, Schaich L, et al. Safety and efficacy of diclofenac sodium 0.1% ophthalmic solution in acute seasonal allergic conjunctivitis. J Ocul Pharmacol Ther 1995;11(3):361-368. (Randomized, controlled trial; 20 patients)
-
Ballas Z, Blumenthal M, Tinkelman DG, et al. Clinical evaluation of ketorolac tromethamine 0.5% ophthalmic solution for the treatment of seasonal allergic conjunctivitis. Surv Ophthalmol 1993 Jul;38 Suppl:141-148. (Multicenter, randomized, controlled trial; 148 patients)
-
Physicians' Desk Reference. Montvale, NJ: Medical Economics; 2002.
-
* el Hennawi M. A double blind placebo controlled group comparative study of ophthalmic sodium cromoglycate and nedocromil sodium in the treatment of vernal keratoconjunctivitis. Br J Ophthalmol 1994 May;78(5):365-369. (Randomized, controlled trial; 138 patients)
-
Kray KT, Squire EN Jr, Tipton WR, et al. Cromolyn sodium in seasonal allergic conjunctivitis. J Allergy Clin Immunol 1985 Oct;76(4):623-627. (Randomized, controlled trial; 58 patients)
-
Verin PH, Dicker ID, Mortemousque B. Nedocromil sodium eye drops are more effective than sodium cromoglycate eye drops for the long-term management of vernal keratoconjunctivitis. Clin Exp Allergy 1999 Apr;29(4):529-536. (Randomized, controlled trial; 34 children)
-
* Henshaw K, Sheikh A, Smeeth L, et al. Mast cell stabilizers for seasonal and perennial allergic conjunctivitis. Cochrane Review. The Cochrane Library, Issue 3, 2001. (Systematic review)
-
Pflugfelder SC. Advances in the diagnosis and management of keratoconjunctivitis sicca. Curr Opin Ophthalmol 1998 Aug;9(4):50-53. (Review)
-
* Care of the Patient with Ocular Surface Disease. American Optometric Association. 1995 (reviewed 1997). (Clinical practice guideline)
-
* Blepharitis. Preferred Practice Pattern. American Academy of Ophthalmology. 1998 Sept. (Clinical practice guideline)
-
Frucht-Pery J, Solomon A, Siganos CS, et al. Treatment of inflamed pterygium and pinguecula with topical indomethacin 0.1% solution. Cornea 1997 Jan;16(1):42-47. (Randomized, controlled trial; 51 patients)
-
Frucht-Pery J, Siganos CS, Solomon A, et al. Topical indomethacin solution versus dexamethasone solution for treatment of inflamed pterygium and pinguecula: a prospective randomized clinical study. Am J Ophthalmol 1999 Feb;127(2):148-152. (Randomized, controlled trial; 51 patients)
-
Chiapella AP, Rosenthal AR. One year in an eye casualty clinic. Br J Ophthalmol 1985 Nov;69(11):865-870. (Observational; 6576 patients)
-
* Flynn CA, D'Amico F, Smith G. Should we patch corneal abrasions? A meta-analysis. J Fam Pract 1998 Oct;47(4):264-270. (Meta-analysis)
-
Kaiser PK, Pineda R 2nd. A study of topical nonsteroidal antiinflammatory drops and no pressure patching in the treatment of corneal abrasions. Corneal Abrasion Patching Study Group. Ophthalmology 1997 Aug;104(8):1353-1359. (Randomized, blinded, placebo-controlled trial; 100 patients)
-
Szucs PA, Nashed AH, Allegra JR, et al. Safety and efficacy of diclofenac ophthalmic solution in the treatment of corneal abrasions. Ann Emerg Med 2000 Feb;35(2):131-137. (Randomized, controlled trial; 49 patients)
-
* Clemons CS, Cohen EJ, Arentsen JJ, et al. Pseudomonas ulcers following patching of corneal abrasions associated with contact lens wear. CLAO J 1987 May;13(3):161-164. (Retrospective, case report)
-
* Schein OD. Contact lens abrasions and the nonophthalmologist. Am J Emerg Med 1993 Nov;11(6):606-608. (Case report)
-
Pepose JS, Wilhelmus KR. Divergent approaches to the management of corneal ulcers. Am J Ophthalmol 1992;114: 630-632. (Review)
-
* Cheung J, Slomovic AR. Microbial etiology and predisposing factors among patients hospitalized for corneal ulceration. Can J Ophthalmol 1995 Aug;30(5):251-255. (Case report)
-
Bacterial Keratitis. Preferred Practice Pattern. American Academy of Ophthalmology. 2000 Sept. (Clinical practice guideline)
-
Benson WH, Lanier JD. Current diagnosis and treatment of corneal ulcers. Curr Opin Ophthalmol 1998 Aug;9(4):45-49. (Systematic review)
-
No authors listed. Ofloxacin monotherapy for the primary treatment of microbial keratitis: a double-masked, randomized, controlled trial with conventional dual therapy. The Ofloxacin Study Group. Ophthalmology 1997 Nov;104(11):1902-1909. (Multicenter, randomized, blinded, trial; 122 patients)
-
Hyndiuk RA, Eiferman RA, Caldwell DR, et al. Comparison of ciprofloxacin ophthalmic solution 0.3% to fortified tobramycincefazolin in treating bacterial corneal ulcers. Ciprofloxacin Bacterial Keratitis Study Group. Ophthalmology 1996 Nov;103(11):1854-1862; discussion 1862-1863. (Multicenter, randomized, controlled trial; 324 patients)
-
* Goldstein MH, Kowalski RP, Gordon YJ. Emerging fluoroquinolone resistance in bacterial keratitis: a 5-year review. Ophthalmology 1999;106:1313-1318. (Review)
-
Walton RC, Nussenblatt RB. Anterior uveitis. In: Krachmer JH, Mannis MJ, Holland E, eds. Cornea. St. Louis: Mosby; 1997:1493-1503. (Textbook chapter)
-
As cited in: The Columbia World of Quotations, 1996.
-
* Pavan-Langston D. Herpes simplex of the ocular anterior segment. Curr Clin Top Infect Dis 2000;20:298-324. (Review)
-
* Gaynor BD, Margolis TP, Cunningham ET Jr. Advances in diagnosis and treatment of herpetic uveitis. Int Ophthalmol Clin 2000 Spring;40(2):85-109. (Systematic review)
-
No authors listed. Acyclovir for the prevention of recurrent herpes simplex virus eye disease. Herpetic Eye Disease Study Group. N Engl J Med 1998 Jul 30;339(5):300-306. (Multicenter, randomized, controlled trial; 703 patients)
-
Harding SP, Lipton JR, Wells JC. Natural history of herpes zoster ophthalmicus: predictors of postherpetic neuralgia and ocular involvement. Br J Ophthalmol 1987;71:353-358. (Review)
-
Cobo LM, Foulks GN, Liesegang T, et al. Oral acyclovir in the treatment of acute herpes zoster ophthalmicus. Ophthalmology 1986 Jun;93(6):763-770. (Randomized, controlled trial; 71 patients)
-
* Klotz SA, Penn CC, Negvesky GJ, et al. Fungal and parasitic infections of the eye. Clin Microbiol Rev 2000 Oct;13(4): 662-685. (Review)
-
Bozeman W. Acute angle-closure glaucoma. In: Harwood-Nuss A, et al, eds. The Clinical Practice of Emergency Medicine. Philadelphia: Lippincott Williams & Wilkins; 2000:67-71. (Textbook chapter)
-
Ritch R, Lowe RF, et al, eds. The Glaucomas. St. Louis: Mosby; 1989. (Textbook)
-
Coleman AL. Glaucoma. Lancet 1999 Nov 20;354(9192): 1803-1810. (Review)
-
* Ritch R, Lowe RF. Angle-closure glaucoma: therapeutic overview. In: Ritch R, et al, eds. The Glaucomas. St. Louis: Mosby; 1996. Chapter 74. (Textbook chapter)
-
Pavesio CE, Meier FM. Systemic disorders associated with episcleritis and scleritis. Ophthalmology 2001;12(6): 471-478. (Review)
-
McMullen M, Kovarik G, Hodge WG. Use of topical steroid therapy in the management of nonnecrotizing anterior cleritis. Can J Ophthalmol 1999 Jun;34(4):217-221. (Phase I/II descriptive study; 32 patients)
-
* Jabs DA, Mudun A, Dunn JP, et al. Episcleritis and scleritis: clinical features and treatment results. Am J Ophthalmol 2000 Oct;130(4):469-476. (Retrospective; 134 patients)
-
Akpek EK, Uy HS, Christen W, et al. Severity of episcleritis and systemic disease association. Ophthalmology 1999 Apr;106(4):729- 731. (Retrospective; 100 patients)
-
Honig MA, Rapuano CJ. Management of corneal perforation. In: Krachmer JH, Mannis MJ, Holland E, eds. Cornea. St. Louis: Mosby; 1997:1817. (Textbook chapter)
-
* Wald ER. Conjunctivitis in infants and children. Pediatr Infect Dis J 1997;16(2 Suppl):S17-S20. (Review)
-
Weiss A. Acute conjunctivitis in childhood. Curr Probl Pediatr 1994;24(1):4-11. (Review)
-
* Bodor FF, Marchant CD, Shurin PA, et al. Bacterial etiology of conjunctivitis-otitis media syndrome. Pediatrics 1985 Jul;76(1):26-28. (Prospective descriptive series, convenience sample; 20 episodes)
-
Lueder GT. Neonatal dacryocystitis associated with nasolacrimal duct cysts. J Pediatr Ophthalmol trabismus 1995 Mar;32(2):102-106. (Prospective, case report; 3 patients)
-
Gross RD, Hoffman RO, Lindsay RN. A comparison of ciprofloxacin and tobramycin in bacterial conjunctivitis in children. Clin Pediatr (Phila) 1997 Aug;36(8):435-444. (Randomized, controlled trial; 257 children)
-
Wald ER, Serdy C, Guerra N, et al. Short course: oral antibiotic treatment of bacterial conjunctivitis [Abstract 727]. Program and abstracts of the American Pediatric Society-The Society for Pediatric Research Annual Meeting, Washington, DC, May 3 to 6, 1993. Pediatr Res 1993;33:124A.
-
Bodor FF. Systemic antibiotics for treatment of the conjunctivitisotitis media syndrome. Pediatr Infect Dis J 1989 May;8(5):287-290. (114 episodes)
-
Harrison CJ, Hedrick JA, Block SL, et al. Relation of the outcome of conjunctivitis and the conjunctivitis-otitis syndrome to identifiable risk factors and oral antimicrobial therapy. Pediatr Infect Dis J 1987 Jun;6(6):536-540. (Randomized, controlled trial; 83 patients)
-
* The American Academy of Pediatrics. Chlamydial infections, gonococcal infections, herpes simplex infections, meningococcal infections and Kawasaki disease. In: Pickering LK, ed. 2000 Red Book: Report of the Committee on Infectious Diseases, 25th ed. Elk Grove Village, IL: American Academy of Pediatrics: 1997;208-212, 254-260, 309-313, 360-363, 396-401, 650-656. (Textbook)
-
* Shovlin JP. Orbital infections and inflammations. Curr Opin Ophthalmol 1998 Oct;9(5):41-48. (Review)
-
Rumelt S, Rubin PA. Potential sources for orbital cellulitis. Int Ophthalmol Clin 1996 Summer;36(3):207-221. (Review)
-
Phillips PH. The orbit. Ophthalmol Clin North Am 2001 Mar;14(1):109-127, viii. (Systematic review)
-
* Barone SR, Aiuto LT. Periorbital and orbital cellulitis in the Haemophilus influenzae vaccine era. J Pediatr Ophthalmol Strabismus 1997 Sep;34(5):293-296. (Retrospective; 134 patients)
-
Schwartz GR, Wright SW. Changing bacteriology of periorbital cellulitis. Ann Emerg Med 1996 Dec;28(6):617-620. Retrospective; 49 patients)
-
* Powell KR. Orbital and periorbital cellulitis. Pediatr Rev 1995;16(5):163-167. (Review)
-
* Dudin A, Othman A. Acute periorbital swelling: evaluation of management protocol. Pediatr Emerg Care 1996 Feb;12(1):16-20. (Evaluation; 34 patients)
-
* No authors listed; American Academy of Pediatrics. Subcommittee on Management of Sinusitis and Committee on Quality Improvement Clinical practice guideline: management of sinusitis. Pediatrics 2001 Sep;108(3):798-808. (Clinical practice guideline; 79 references)
-
Alteveer JG, McCans K. Pediatric eye disorders. In: Harwood- Nuss A, et al, eds. The Clinical Practice of Emergency Medicine. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2000:1246. (Textbook chapter)
-
Personal communication with Deborah Meislich, MD, Pediatric Infectious Disease, Cooper Hospital/UMC, Camden, NJ.
-
Sharma S. Ophthaproblem. Congenital nasolacrimal duct obstruction. Can Fam Physician 1998 Oct;44:2085, 2095. (Case report)
-
* Pollard ZF. Treatment of acute dacryocystitis in neonates. J Pediatr Ophthalmol Strabismus 1991 Nov;28(6):341-343. (25 newborns)
-
Campolattaro BN, Lueder GT, Tychsen L. Spectrum of pediatric dacryocystitis: medical and surgical management of 54 cases. J Pediatr Ophthalmol Strabismus 1997 May;34(3):143-153. (Case report; 54 patients)
-
Donahue SP, Khoury JM, Kowalski RP. Common ocular infections. A prescriber's guide. Drugs 1996 Oct;52(4):526-540. (Review)
-
* Laskowitz D, Liu GT, Galetta SL. Acute visual loss and other disorders of the eyes. Neurol Clin 1998 May;16(2):323-353. (Systematic review)
-
Young PA, Young PH. Basic Clinical Neuroanatomy. Baltimore: Williams & Wilkins; 1997. (Textbook)
-
Burde RM, Savino PJ, Trobe JD. Clinical Decisions in Neuro- Ophthalmology. St Louis: Mosby; 1992. (Textbook)
-
* Morgan A, Hemphill RR. Acute visual change. Emerg Med Clin North Am 1998 Nov;16(4):825-843, vii. (Review)
-
Morris RJ. Double vision as a presenting symptom in an ophthalmic casualty department. Eye 1991;5(Pt 1):124-129. (Prospective; 275 patients)
-
Eggenberger ER. Inflammatory optic neuropathies. Ophthalmol Clin North Am 2001 Mar;14(1):73-82. (Systematic review)
-
Rodriguez M, Siva A, Cross SA, et al. Optic neuritis: a populationbased study in Olmsted County, Minnesota. Neurology 1995 Feb;45(2):244-250. (Retrospective; 156 patients)
-
Beck RW, Cleary PA, Trobe JD, et al. The effect of corticosteroids for acute optic neuritis on the subsequent development of multiple sclerosis. The Optic Neuritis Study Group. N Engl J Med 1993 Dec 9;329(24):1764-1769. (Multicenter, randomized, controlled trial; 389 patients)
-
* Granadier RJ. Ophthalmology update for primary practitioners. Part I. Update on optic neuritis. Dis Mon 2000 Aug;46(8):508- 532. (Review)
-
No authors listed. Acute methanol poisoning ‘the blind drunk'. West J Med 1981 Aug;135(2):122-128. (Case report)
-
Jacobsen D. Methanol poisoning. In: Harwood-Nuss A, et al, eds. The Clinical Practice of Emergency Medicine. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2000:1542. (Textbook chapter)
-
* Beatty S, Au Eong KG. Acute occlusion of the retinal arteries: current concepts and recent advances in diagnosis and management. J Accid Emerg Med 2000 Sep;17(5):324-329. (Systematic review)
-
Cooney MJ, Fekrat S, Finkelstein D. Current concepts in the management of central retinal vein occlusion. Curr Opin Ophthalmol 1998 Jun;9(3):47-50. (Review)
-
* Bhagat N, Goldberg MF, Gascon P, et al. Central retinal vein occlusion: review of management. Eur J Ophthalmol 1999 Jul;9(3):165-180. (Review)
-
Branum G, Massey EW, Rice J. Erythrocyte sedimentation rate in temporal arteritis. South Med J 1987 Dec;80(12):1527-1528. (Retrospective; 62 patients)
-
* Olitsky SE, Nelson LB. Common ophthalmologic concerns in infants and children. Pediatr Clin North Am 1998;45(4): 993-1012. (Review)
-
The Pediatric Eye Diseases Investigation Group. A randomized trial of Atropine versus patching for the treatment of moderate amblyopia in children. Ophthalmology 2002 Mar;120(3):268-278. (Multicenter, randomized, controlled trial)
-
Repka MX. Common pediatric neuro-ophthalmologic conditions. Pediatr Clin North Am 1993;40(4):777-778. (Review)
-
Morales DS, Siatkowski RM, Howard CW, et al. Optic neuritis in children. J Pediatr Ophthalmol Strabismus 2000 Sep;37(5):254-259. (Retrospective; 15 patients)
-
Brady KM, Brar AS, Lee AG, et al. Optic neuritis in children: clinical features and visual outcome. J AAPOS 1999 Apr;3(2):98- 103. (Retrospective; 25 patients)









 678-366-7933
678-366-7933