Table of Contents
About This Issue
Abnormal uterine bleeding affects nearly one-third of women throughout their lives, ranging from minor to severe. Upon presentation in the urgent care, a comprehensive understanding of the pathophysiology and etiologies of abnormal uterine bleeding is needed to effectively manage these patients. In this issue, you will learn:
How the history and physical examination can identify the cause of bleeding
What the most current medical therapies are available for abnormal uterine bleeding
When it is appropriate to treat patients with abnormal uterine bleeding in the urgent care setting, refer to a gynecologist, or refer to the emergency department for further evaluation
CODING & CHARTING: Detailed documentation of the level of severity of abnormal uterine bleeding will contribute to accurate coding. Learn more in our monthly coding column.
- About This Issue
- Abstract
- Case Presentations
- Abbreviations
- Introduction
- Etiology and Pathophysiology
- The PALM-COEIN Classification System
- Differential Diagnosis
- Girls Aged 12 to 18 Years
- Women Aged 19 to 39 Years
- Women Aged 40 Years and Older
- Urgent Care Evaluation
- Initial Evaluation of Bleeding
- History
- Physical Examination
- Diagnostic Studies
- Pregnancy Test
- Complete Blood Count
- Coagulation Studies
- Other Studies
- Imaging Studies
- Treatment
- Management of the Stable Patient
- Hormonal Therapies
- Combination Oral Contraceptive Pills
- Oral Progestin
- Nonhormonal Therapies
- Transfusion of Packed Red Blood Cells
- Nonsteroidal Anti-inflammatory Drugs
- Tranexamic Acid
- Nonsurgical Treatment Summary
- Management of the Unstable Patient
- Surgical Treatment
- Special Populations and Situations
- Patients Taking Direct Oral Anticoagulants
- Prepubescent Girls
- Genital Injuries
- Accidental Injuries
- Intentional Injuries
- Sexual Abuse and Assault
- Controversies and Cutting Edge
- Levonorgestrel-Releasing Intrauterine System
- Elagolix
- Disposition
- Summary
- Risk Management Pitfalls for Abnormal Uterine Bleeding in Nonpregnant Patients
- Time- and Cost-Effective Strategies
- Critical Appraisal of The Literature
- KidBits: Abnormal Uterine Bleeding in Children
- Overview By Age Group
- Neonate (Aged <30 Days)
- Premenarchal (Aged 30 Days-10 Years)
- Menarche (Aged 10+ Years)
- History and Physical Examination
- Differential Diagnosis
- Vulvovaginitis
- Foreign Body
- Infections
- Autoimmune/Endocrine/Genetic
- Anatomic
- Key Points
- References
- Sexual Abuse Considerations
- Case Conclusions
- Coding & Charting: What You Need to Know
- Number and Complexity of Problems Addressed
- Amount and/or Complexity of Data to be Reviewed and Analyzed
- Risk of Complications and/or Morbidity or Mortality of Patient Management
- Coding Challenge: Abnormal Uterine Bleeding in Urgent Care
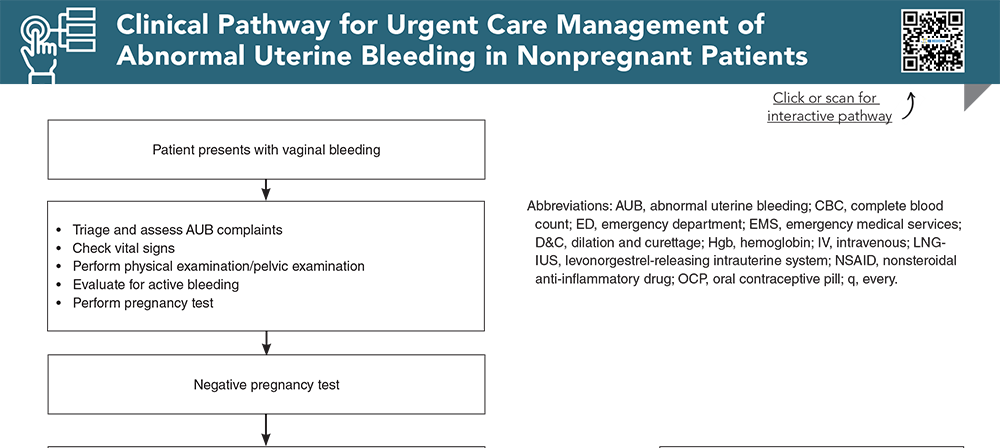
- Clinical Pathway for Urgent Care Management of Abnormal Uterine Bleeding in Nonpregnant Patients
- References
Abstract
Uterine bleeding that is abnormal in timing, duration, or quantity affects nearly one-third of women and carries a substantial financial and quality-of-life burden. An estimated 5% of emergency visits are for vaginal bleeding, and 1% of those patients will have a life-threatening cause that must be identified. These patients may also present to urgent care, and urgent care clinicians need to have a comprehensive understanding of the pathophysiology and etiologies of abnormal uterine bleeding to effectively manage these patients. This issue reviews the common causes and clinical approach to abnormal uterine bleeding in nonpregnant patients from prepubescence through menopause.
Case Presentations
- The patient states that she has been unable to get an appointment with her gynecologist until the end of the week, and she is concerned over the increasing blood loss.
- She has a history of irregular menstrual periods, and she was having intermittent spotting that has become heavier, with clots, over the past 5 days. She is using multiple pads a day.
- In triage, her vital signs are within normal limits. You order a pregnancy test, which is negative.
- You wonder whether and how you should begin treatment, or whether you should do nothing and defer to her gynecologist…
- The patient appears pale and weak and her heart is racing. Her mother says that she almost fainted on the way over. Your staff becomes anxious when they see this young patient come into the urgent care.
- She tells you that she began spotting 1 week prior, but the bleeding has become acutely worse. Her mother notes that the patient told her that she had a nosebleed a few days ago.
- You quickly assess the patient and consider a treatment plan to best care for this patient…
- She has been taking hormone replacement therapy for the last year but has not had any problems.
- Her medical history is remarkable for obesity, hypertension, and diabetes.
- Initial assessment in the urgent care reveals stable vital signs. An abdominal examination is normal. The pelvic examination is remarkable for a small amount of old blood in the vaginal vault with no other abnormalities of the cervix or vagina.
- The bimanual examination reveals a small nontender uterus with no adnexal masses or tenderness.
- You consider the best course of action for this patient, considering her risk factors and clinical presentation...
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
Clinical Pathway for Urgent Care Management of Abnormal Uterine Bleeding in Nonpregnant Patients
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Buy this issue and
CME test to get 4 CME credits.
Key References
Following are the most informative references cited in this paper, as determined by the authors.
1. * Munro MG, Critchley HOD, Fraser IS. The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions. Int J Gynaecol Obstet. 2018;143(3):393-408. (Practice guidelines) DOI: 10.1002/ijgo.12666
2. * Levy-Zauberman Y, Pourcelot AG, Capmas P, et al. Update on the management of abnormal uterine bleeding. J Gynecol Obstet Hum Reprod. 2017;46(8):613-622. (Practice guidelines) DOI: 10.1016/j.jogoh.2017.07.005
21. * Borhart J. Emergency department management of vaginal bleeding in the nonpregnant patient. Emerg Med Pract. 2013;15(8):1-20. (Practice guideline) PMID: 24044770
26. * Bofill Rodriguez M, Lethaby A, Low C, et al. Cyclical progestogens for heavy menstrual bleeding. Cochrane Database Syst Rev. 2019;8(8):CD001016. (Systematic review) DOI: 10.1002/14651858.cd001016.pub3
46. * Lopez HN, Focseneanu MA, Merritt DF. Genital injuries acute evaluation and management. Best Pract Res Clin Obstet Gynaecol. 2018;48:28-39. (Review) DOI: 10.1016/j.bpobgyn.2017.09.009
48. * Lethaby A, Hussain M, Rishworth JR, et al. Progesterone or progestogen-releasing intrauterine systems for heavy menstrual bleeding. Cochrane Database Syst Rev. 2015(4):CD002126. (Systematic review) DOI: 10.1002/14651858.cd002126.pub4
Subscribe to get the full list of 48 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: abnormal uterine bleeding, heavy menstrual bleeding, dysfunctional uterine bleeding, and nonpregnant vaginal bleeding, menorrhagia, ovulatory dysfunction









 678-366-7933
678-366-7933