Table of Contents
About This Issue
Pediatric penile problems range from congenital anomalies to acquired and emergent conditions that require prompt recognition and management. Emergency clinicians must be comfortable evaluating these sensitive presentations across all pediatric age groups, from neonates with postcircumcision bleeding to adolescents with paraphimosis or priapism. This issue presents a structured, evidence-based approach to the diagnosis and management of common pediatric penile problems, with emphasis on pain management, recognizing emergent conditions, and timely urologic consultation. In this issue, you will learn:
How to distinguish emergent from nonemergent pediatric penile conditions and to identify indications for immediate urologic consultation
Evidenced-based recommendations for selecting appropriate systemic, local, and regional analgesia, and when anxiolytic medications or procedural sedation are indicated
Guidance for recognizing and managing infectious and inflammatory conditions, including balanitis, balanoposthitis, and urethritis
How to classify and treat priapism, including techniques for corporeal aspiration and intracavernosal sympathomimetic injection
Recommendations for managing strangulation conditions, including hair tourniquet removal and manual reduction of paraphimosis
Recommendations for evaluating and managing traumatic and surgical injuries, including straddle injuries, zipper entrapment, penile fracture, and postcircumcision bleeding
How to screen for nonaccidental trauma and when to involve Child Protective Services or a child abuse team
- About This Issue
- Abstract
- Case Presentations
- Introduction
- Critical Appraisal of the Literature
- Etiology and Pathophysiology
- Differential Diagnosis
- Congenital Penile Conditions
- Acquired Penile Conditions
- Infectious and Inflammatory Conditions
- Hematologic Conditions
- Strangulation Conditions
- Trauma and Surgical Injuries
- Prehospital Care
- Emergency Department Evaluation
- History
- Physical Examination
- Diagnostic Studies
- Laboratory Studies
- Imaging Studies
- Treatment
- General Principles
- Pain Management
- Anxiolytic Medications and Sedation
- Diagnosis-Specific Treatment
- Congenital Penile Conditions
- Acquired Penile Conditions
- Infectious and Inflammatory Conditions
- Hematologic Conditions
- Strangulation Conditions
- Hair Tourniquet
- Paraphimosis
- Trauma and Surgical Injuries
- Zipper Entrapment
- Straddle Injury
- Penile Fracture
- Postcircumcision Bleeding
- Special Considerations
- Controversies and Cutting Edge
- Disposition
- General Considerations
- Consultation
- Infectious and Inflammatory Conditions
- Hematologic Conditions
- Strangulation Conditions
- Trauma and Surgical Injuries
- Zipper Entrapment
- Straddle Injury
- Penile Fracture
- Postcircumcision Bleeding
- Summary
- 5 Things That Will Change Your Practice
- Risk Management Pitfalls for Emergency Department Management of Pediatric Patients With Penile Problems
- Time- and Cost-Effective Strategies
- Case Conclusions
- Clinical Pathway for Evaluation and Management of a Child With a Penile Problem in the Emergency Department
- Tables and Figures
- References
Abstract
Pediatric penile problems range from congenital anomalies to acquired and emergent conditions. Acquired conditions can result from various causes, including infectious and inflammatory conditions, hematologic conditions, strangulation conditions, trauma, and surgical injuries. This review provides an overview of the presentation, diagnosis, and management of pediatric penile problems that may present to the emergency department. Recommendations are given for evaluation and management, with emphasis on pain relief, restoration of normal anatomy, and timely treatment. Guidance is also provided on indications for emergent urologic consultation. Optimizing outcomes for pediatric patients with penile conditions requires addressing key challenges, including effective pain and anxiety management, thoughtful use of imaging, and careful evaluation for possible abuse.
Case Presentations
- The boy was born at full term with no complications. The parents tell you the circumcision was completed without complications at the delivering hospital prior to discharge. Since the procedure, they have seen a “significant amount” of bright-red blood with each diaper change. They have been applying petroleum jelly as directed. There is no family history of bleeding diatheses. The baby received vitamin K after delivery. The newborn screen is pending.
- On examination, there is a small amount of bright-red blood dripping from the circumcision site.
- What workup is warranted at this time, and what are the next steps in management?
- The boy has no prior history of urinary tract infections. He is toilet-trained. His parents report dribbling of urine for the last few days and inability to void when attempting to urinate.
- On examination, there is edema and ballooning of the foreskin of the penis. The foreskin is unable to be retracted to visualize the tip of the penis; however, there is scant discharge from the end of the penis. There are a few erythematous “satellite lesions” on the inguinal creases. His urine is positive for 1+ leukocytes and negative for nitrites.
- What is the appropriate management for this patient?
- The boy takes no medications and denies being sexually active.
- The physical examination is notable for a donut-shaped, erythematous, and exquisitely painful circumferential swelling at the base of the glans, with moderate swelling of the glans and flaccidity proximal to it. There is no discharge.
- What pain control measures and techniques should be considered for management of this patient’s condition?
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
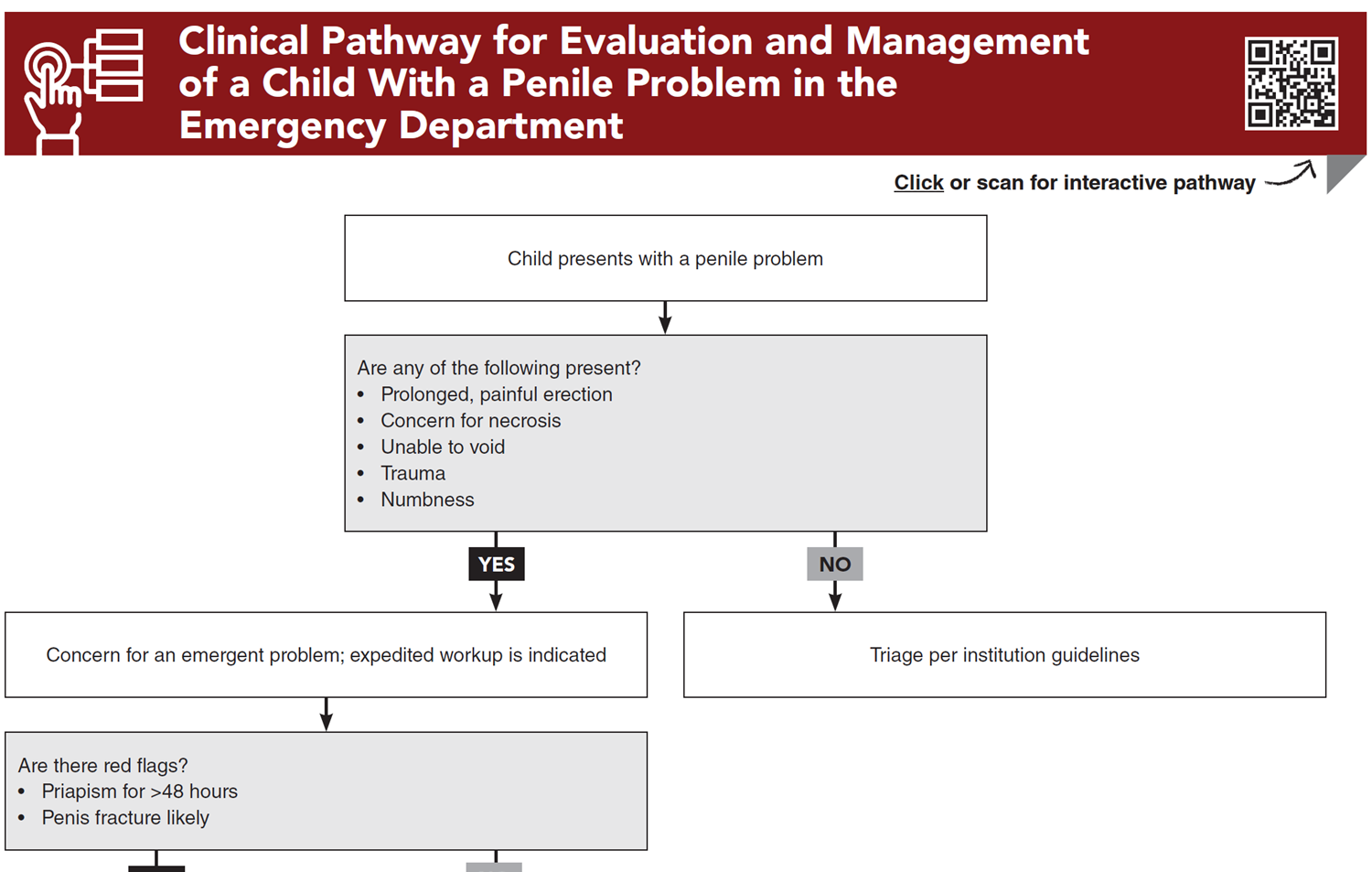
Clinical Pathway for Evaluation and Management of a Child With a Penile Problem in the Emergency Department
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Tables and Figures
Subscribe for full access to all Tables and Figures.
Buy this issue and
CME test to get 4 CME credits.
Key References
Following are the most informative references cited in this paper, as determined by the authors.
8. * Chan IH, Wong KK. Common urological problems in children: prepuce, phimosis, and buried penis. Hong Kong Med J. 2016;22(3):263-269. (Review) DOI: 10.12809/hkmj154645
11. * Donaldson JF, Rees RW, Steinbrecher HA. Priapism in children: a comprehensive review and clinical guideline. J Pediatr Urol. 2014;10(1):11-24. (Review) DOI: 10.1016/j.jpurol.2013.07.024
16. * Leslie JA, Cain MP. Pediatric urologic emergencies and urgencies. Pediatr Clin North Am. 2006;53(3):513-527. (Review) DOI: 10.1016/j.pcl.2006.02.007
23. * McGrath NA, Howell JM, Davis JE. Pediatric genitourinary emergencies. Emerg Med Clin North Am. 2011;29(3):655-666. (Review) DOI: 10.1016/j.emc.2011.04.003
34. * Morey AF, Metro MJ, Carney KJ, et al. Consensus on genitourinary trauma: external genitalia. BJU Int. 2004;94(4):507-515. (Review) DOI: 10.1111/j.1464-410X.2004.04993.x
49. * Adjei NN, Lynn AY, Grimshaw A, et al. Systematic literature review of pediatric male and female genital hair thread tourniquet syndrome. Pediatr Emerg Care. 2022;38(2):e799-e804. (Literature review) DOI: 10.1097/PEC.0000000000002383
58. * Hobbs CJ, Osman J. Genital injuries in boys and abuse. Arch Dis Child. 2007;92(4):328-331. (Review) DOI: 10.1136/adc.2006.111195
Subscribe to get the full list of 59 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: pediatric penile problems, phimosis, paraphimosis, priapism, balanitis, balanoposthitis, urethritis, hair tourniquet, zipper entrapment, straddle injury, penile fracture, postcircumcision bleeding, hypospadias, epispadias, chordee, buried penis, pediatric genitourinary emergency, penile block, corporeal aspiration, sickle cell priapism, nonaccidental trauma, pediatric urology










 678-366-7933
678-366-7933