

|
|
Pediatric dehydration is a top concern that leads parents to bring their children into the emergency department for evaluation. Rehydration therapy should be tailored to the severity of illness, available resources, and the child’s clinical status. Although accurately determining the fluid deficit can be challenging, guidance is provided for use of scoring systems to estimate the degree of dehydration. Recommendations are given for first-line oral rehydration therapy, and for rehydration through intravenous, intraosseous, or subcutaneous methods when oral rehydration is not an option. A thoughtful, goal-directed approach that emphasizes timely rehydration, caregiver education, and careful follow-up can improve outcomes.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
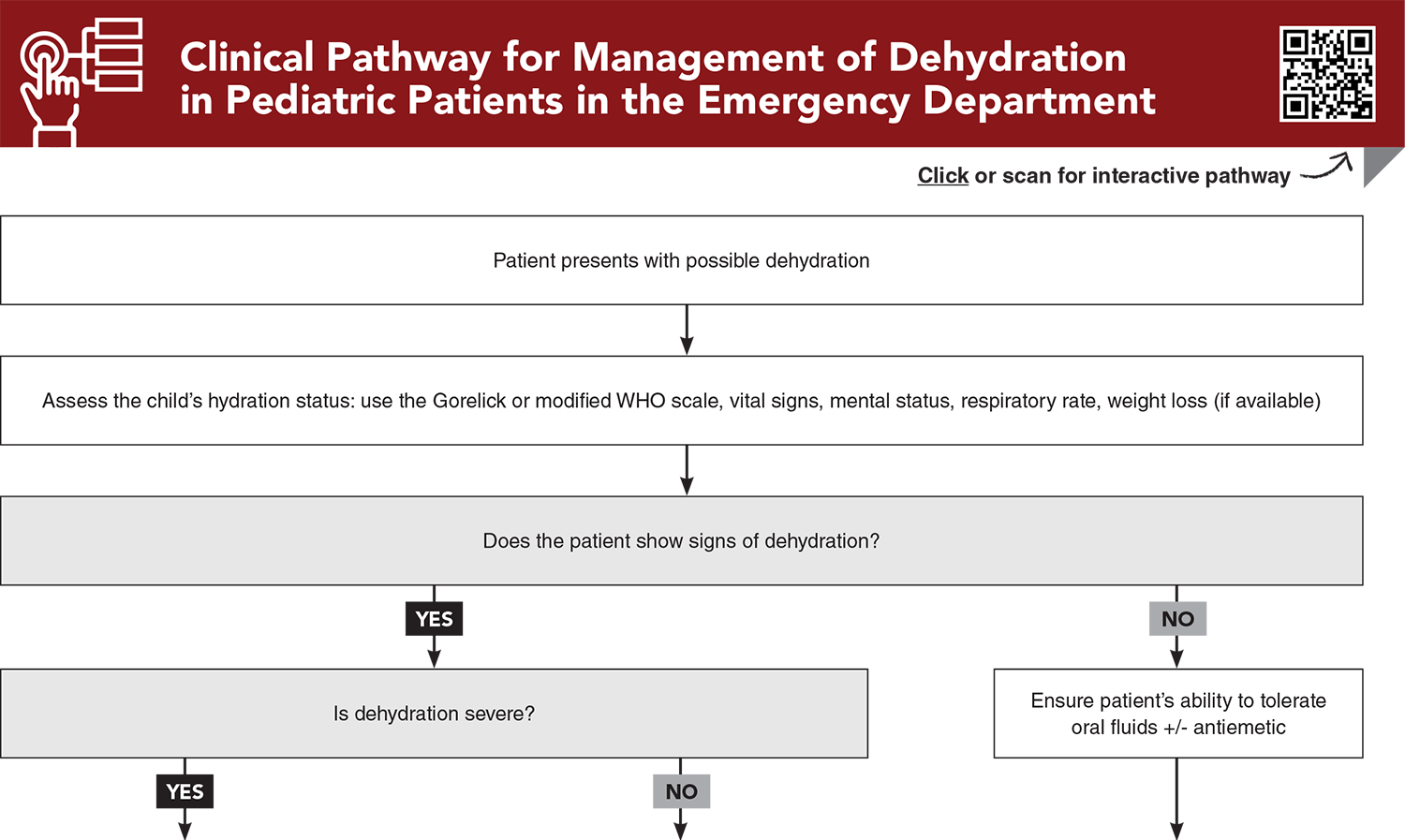
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
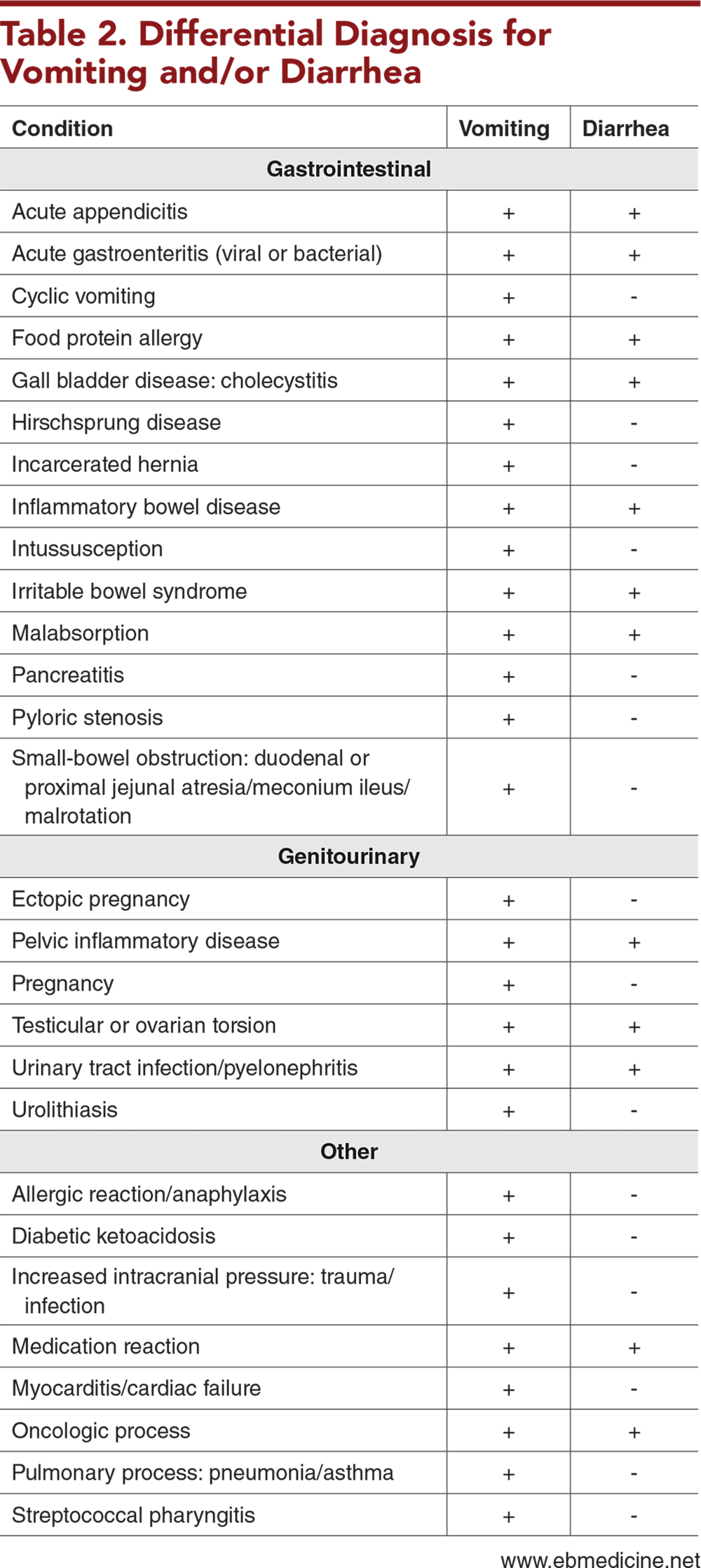
Subscribe for full access to all Tables.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
2. * Gorelick MH, Shaw KN, Murphy KO. Validity and reliability of clinical signs in the diagnosis of dehydration in children. Pediatrics. 1997;99(5):E6. (Prospective cohort study; 186 children) DOI: 10.1542/peds.99.5.e6
3. * Steiner MJ, DeWalt DA, Byerley JS. Is this child dehydrated? JAMA. 2004;291(22):2746-2754. (Systematic review; 13 studies) DOI: 10.1001/jama.291.22.2746
9. * Levine AC, Gainey M, Qu K, et al. A comparison of the NIRUDAK models and WHO algorithm for dehydration assessment in older children and adults with acute diarrhoea: a prospective, observational study. Lancet Glob Health. 2023;11(11):e1725-e1733. (Prospective observational study; 1580 patients) DOI: 10.1016/S2214-109X(23)00403-5
14. * Wathen JE, MacKenzie T, Bothner JP. Usefulness of the serum electrolyte panel in the management of pediatric dehydration treated with intravenously administered fluids. Pediatrics. 2004;114(5):1227-1234. (Prospective study; 182 patients) DOI: 10.1542/peds.2004-0457
16. * Nagler J, Wright RO, Krauss B. End-tidal carbon dioxide as a measure of acidosis among children with gastroenteritis. Pediatrics. 2006;118(1):260-267. (Prospective study; 130 patients) DOI: 10.1542/peds.2005-2723
Subscribe to get the full list of 42 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: dehydration, vomiting, diarrhea, fluid deficit, fluid loss, rehydration, fluid resuscitation, oral rehydration therapy, oral rehydration solution, intravenous therapy, subcutaneous hydration, nasogastric hydration, total body water, capillary refill, skin turgor, skin elasticity, respiratory pattern, classification of dehydration, clinical dehydration scale, Gorelick Scale, World Health Organization, WHO, Novel Innovative Research for Understanding Dehydration in Adults and Kids, NIRUDAK, Dehydration: Assessing Kids Accurately, DHAKA, urine specific gravity, serum electrolytes, serum bicarbonate, point-of-care ultrasound, goal-directed therapy, BRAT diet, zinc, probiotics
Christopher S. Amato, MD, FAAP, FACEP
Nicole Gerber, MD; Matthew Wilkinson, MD, MPH, FAAP, FACEP
January 1, 2026
January 1, 2029 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAP Prescribed Credits, 4 AOA Category 2-B Credits. Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 0.5 Pharmacology CME credits, subject to your state and institutional approval.
Pediatric Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Pediatric Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933