

|
|
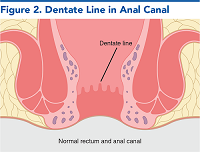
Rectal bleeding accounts for approximately 1 out of every 1000 United States emergency department visits annually. The causes of rectal bleeding are broad, and can range from the benign to the life-threating. This review provides foundational knowledge on rectal bleeding as well as evidence-based recommendations for its evaluation and initial management in the emergency department. Anatomic considerations are discussed, and the differential diagnosis based on risk factors such as age and comorbid conditions is presented. Treatment recommendations based on the presumed diagnosis as well as the evidence associated with their use are also described. Decision-making, including disposition based on laboratory results, imaging studies, and application of risk scoring calculations is also discussed.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.

Subscribe to access the complete flowchart to guide your clinical decision making.




Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
4. * Kocaoğlu S, Çetinkaya HB. Use of age shock index in determining severity of illness in patients presenting to the emergency department with gastrointestinal bleeding. Am J Emerg Med. 2021;47:274-278. (Retrospective; 151 patients) DOI: 10.1016/j.ajem.2021.05.008
18. * Harewood GC, McConnell JP, Harrington JJ, et al. Detection of occult upper gastrointestinal tract bleeding: performance differences in fecal occult blood tests. Mayo Clin Proc. 2002;77(1):23-28. (Prospective; 42 patients) DOI: 10.4065/77.1.23
24. * Sengupta N, Feuerstein JD, Jairath V, et al. Management of patients with acute lower gastrointestinal bleeding: an updated ACG guideline. Am J Gastroenterol. 2023;118(2):208-231. (Guidelines) DOI: 10.14309/ajg.0000000000002130
29. * Triantafyllou K, Gkolfakis P, Gralnek IM, et al. Diagnosis and management of acute lower gastrointestinal bleeding: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2021;53(8):850-868. (Society guidelines) DOI: 10.1055/a-1496-8969
30. * Abraham NS, Barkun AN, Sauer BG, et al. American College of Gastroenterology-Canadian Association of Gastroenterology clinical practice guideline: management of anticoagulants and antiplatelets during acute gastrointestinal bleeding and the periendoscopic period. Am J Gastroenterol. 2022;117(4):542-558. (Society guidelines) DOI: 10.14309/ajg.0000000000001627
54. * Oakland K, Jairath V, Uberoid R, et al. Derivation and validation of a novel risk score for safe discharge after acute lower gastrointestinal bleeding: a modelling study. Lancet Gastroenterol Hepatol. 2017 Sep;2(9):635-643. (Prospective; 2336 patients) DOI: 10.1016/S2468-1253(17)30150-4
Subscribe to get the full list of 56 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: gastrointestinal, lower, hemorrhoids, hematochezia, LGIB, anticoagulant, diverticulitis, fissure, transfusion, hemoglobin, nifedipine, elderly, pregnant, Glasgow-Blatchford, Oakland
Benjamin von Schweinitz, MD, FACEP; Justin Pinkston, MD
Duncan Grossman, DO; Avir Mitra, MD
September 1, 2023
September 1, 2026 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933