

|
|
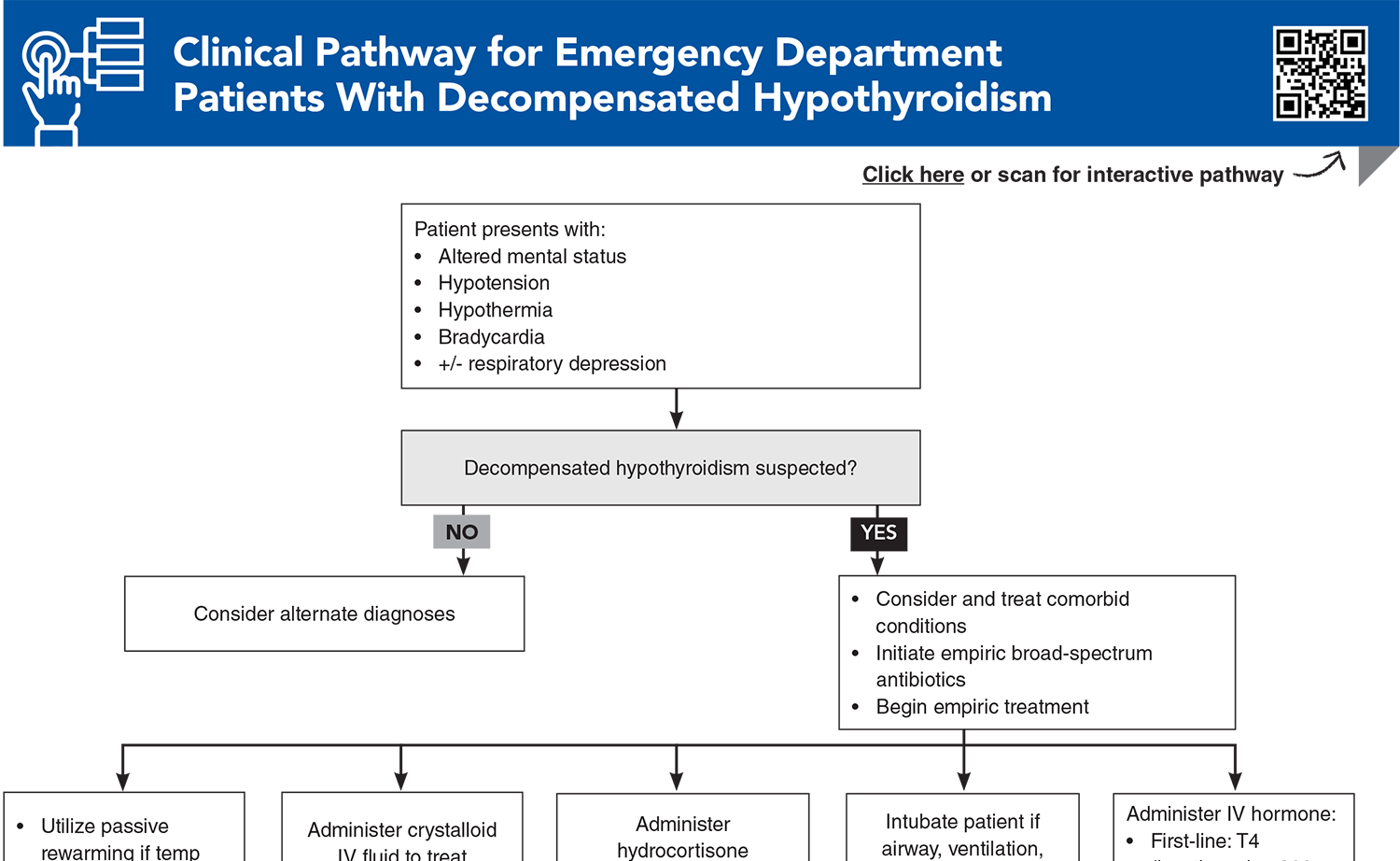
Patients experiencing thyroid emergencies can present with a wide array of clinical presentations and comorbid conditions, so a systematic strategy to identify key historical and physical examination features can help guide the emergency clinician in recognizing these infrequent conditions. This issue review the most up-to-date evidence for diagnosing and managing decompensated hypothyroidism and thyroid storm in adult, pediatric, and pregnant patients.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
1. * Galindo RJ, Hurtado CR, Pasquel FJ, et al. National trends in incidence, mortality, and clinical outcomes of patients hospitalized for thyrotoxicosis with and without thyroid storm in the United States, 2004-2013. Thyroid. 2019;29(1):36-43. (Retrospective longitudinal analysis; 121,384 patients in national database) DOI: 10.1089/thy.2018.0275
3. * Jonklaas J, Bianco AC, Bauer AJ, et al. Guidelines for the treatment of hypothyroidism: prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement. Thyroid. 2014;24(12):1670-1751. (Clinical practice guideline) DOI: 10.1089/thy.2014.0028
4. * Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26(10):1343-1421. (Clinical practice guideline) DOI: 10.1089/thy.2016.0229
5. * Alexander EK, Pearce EN, Brent GA, et al. 2017 Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid. 2017;27(3):315-389. (Clinical practice guideline) DOI: 10.1089/thy.2016.0457
8. * Ono Y, Ono S, Yasunaga H, et al. Clinical characteristics and outcomes of myxedema coma: analysis of a national inpatient database in Japan. J Epidemiol. 2017;27(3):117-122. (Observational study; 149 patients) DOI: 10.1016/j.je.2016.04.002
Subscribe to get the full list of 105 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: hyperthyroidism, thyroid storm, myxedema, thyrotoxicosis, hypothyroidism, Graves, goiter, TSH, T3, T4, hypothermia, tachyarrhythmia, hydrocortisone
Jazmyn J. Shaw, MD; Cindy D. Chang, MD, MEd
Jay Bernstein, MD, MPH, MS, FACEP; Leiloni Kaluhiokalani, DO
June 1, 2025
June 1, 2028 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits. Specialty CME Credits:Included as part of the 4 credits, this CME activity is eligible for 1 Pharmacology CME credit, subject to your state and institutional approval.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933