
|
|
This month's issue of Pediatric Emergency Medicine Practice is the second in a 2-part review of childhood rashes that present to the emergency department. The first part focused on dermatitis and viral and bacterial infections that affect the skin and emphasized the role the emergency physician plays in diagnosing and directing care for these patients.
You're sitting comfortably in the pediatric emergency department of a busy university hospital sipping on hot coffee when you get a phone call from a local physician who's sending you a dilemma that he's been struggling with for over a week. The case is a three-year-old boy with persistent fever over 40oC for eight days, unresponsive to appropriate doses of acetaminophen. The child is very "cranky" and does not seem to want to be coddled by mom; in fact, this seems to make the child more miserable. His eyes are very red, with scant non-purulent discharge for which the pediatrician prescribed antibiotic drops. He has developed a rather impressive truncal rash and swelling of his hands and feet. Blood and urine cultures obtained by the pediatrician have been negative, though his concern for this "irritable" kid was sufficiently worrisome that he elected to start parenteral antibiotics. He's hoping that the resources available in the hospital will help clarify the etiology of this case.
Dermatophytosis, tinea, and ringworm are named according to the site of involvement.6,8-10,15,19,27,28 Tinea capitis, tinea corporis, tinea manum, tinea pedis, tinea cruris, and tinea unguum (onychomycosis) are commonly seen in children and adolescents. Tinea capitis is rarely seen after puberty, whereas tinea pedis and tinea cruris are usually seen in post-pubertal patients. Classically, there is an annular erythematous patch with a leading edge of scale that may be composed of papules and pustules. Clinical suspicion of tinea infection can be confirmed with a KOH preparation; send culture when results are equivocal. The most common offending fungi are microsporum canis and trichophyton mentagrophytes. Wood's light evaluation is not helpful in the diagnosis of suspected lesions on glabrous (hairless) skin. Prescribe topical anti-fungal preparations, such as clotrimazole, miconazole, or tolnaftate, for two weeks; these are usually sufficient for all forms of tinea except for tinea capitis and onychomycosis, where systemic therapy is needed (griseofulvin). The use of topical steroids may mask the diagnosis by amelioration of the signs while the infection persists; this is described by the term "tinea incognito." In tinea corporis, due to microsporum canis, a pet may be the cause of the infection and it may be necessary for the animal to be treated as well.
Tinea pedis may present with a pruritic scale on the lateral and plantar aspects of the feet or maceration between the toes. Inflammation may be minimal, but this infection may progress, leading to pustules, bullae, and swelling which may prove painful. Tinea pedis is a penalty of civilization in that it occurs only in those individuals that wear shoes. Moisture plays a significant role and keeping feet dry (keeping shoes off as much as possible) and changing socks frequently will help.
Tinea manuum is much less common than Tinea pedis and is rarely seen in isolation (the latter occurring concomitantly). It clinically presents on the palms of post-pubertal patients. It is usually unilateral and has morphologic characteristics similar to that seen in Tinea pedis. Involvement of the fingernails frequently occurs in association with Tinea manuum.
Tinea capitis, the most common dermatophytosis of childhood, presents with scaly discrete patches of alopecia with occipital adenopathy. Boys are affected five times more frequently than girls. Endothrix infection, typically caused by microsporum, results in fragile hair and, at times, the hair breaks off at the surface, leaving a "black dot" appearance. Wood's light examination gives a green-blue fluorescence to the infected hair (not skin) when the etiologic agent is microsporum. For KOH preparation, it is important to examine infected hairs. These are usually the fragile broken hairs which are easily removed by gentle traction. Alternatively, scraping the area with a dull scalpel may be needed. Kerion formation can occur as a tender boggy abscess devoid of hair; this is an allergic reaction to the fungus. Treatment consists of a six to eight week course of griseofulvin and a selenium sulfide shampoo (twice weekly) to hasten eradication of spores. It is useful to administer griseofulvin with a fatty meal (milk or ice cream) to aid absorption.
Tinea cruris (jock-itch) resembles tinea infections elsewhere on the body and is most commonly seen in adolescent males. The eruption is sharply marginated and is usually bilaterally symmetrical and involves the intertriginous folds (upper inner thighs). The scrotum is typically spared and its involvement may be suggestive of a candidal infection. Itching is a more consistent feature of Tinea cruris and changes secondary to scratching; excoriation and lichenification are often seen. Tropical climate (perineal sweating) and tight fitting clothes, such as athletic supporters, bathing suits, and panty hose (which prevent evaporation), are contributing factors and avoidance of these helps with treatment. The same anti-fungal preparations mentioned previously can be used to treat Tinea cruris.
Tinea versicolor, caused by a lipophilic yeast named pityrosporum orbiculare, is manifested by tan hypopigmented patches ranging in size from 3-10 cm on areas of the body that have oil producing sebaceous glands, such as the shoulders and upper trunk. Affected areas are hypopigmented because the organism may suppress the formation of melanin or transfer of pigment from melanocytes to keratinocytes. The associated scale may not be readily apparent unless the patch is scratched. In some patients, especially during the winter months, the lesions may be hyperpigmented because of the erythema caused by the fungus. This phenomenon of variable color of the affected skin gives the disease its name. Although the disease is seen most commonly in adolescents (because of their increased levels of sebum production), it may be seen in younger children, typically involving the face. Wood's light examination produces a reddish-brown fluorescence. A KOH preparation shows large clusters of spores and short stubby hyphae, referred to as "meatballs and spaghetti." Treatment consists of lathering the entire body with 2.5% selenium sulfide shampoo which is left on for twenty minutes before washing. Maintenance therapy is recommended because of the high incidence of recurrence. Adolescents may be treated with ketoconozole during the summer months and in recalcitrant cases.

Diaper dermatitis is the most common cutaneous problem of children under two years of age and is provoked by the moist, occluded, irritated environment of the diaper region. Simple irritation of the perineal area (inner thighs, lower abdomen, and buttocks) by stool and urine may lead to shiny erythematous plaques with minimal scale. General treatment principles include using mild soaps, keeping the diaper off as much as possible, and avoiding tightly fitting diapers and rubber pants. There is little literature to support the effectiveness of traditional diaper creams, such as Desitin and A&D ointment, but the efficacy of highly absorbent diapers has been documented in several studies.
C. albicans is found on the skin in 40% of infants with diaper dermatitis within 72 hours of appearance of rash. Furthermore, studies show that this organism is present in less than 10% of infants without pre-existing diaper dermatitis. Monilial diaper dermatitis is characterized by beefy red plaques with a fine white scale and pinpoint satellite papules and pustules on the buttocks and inner thighs. At times, the infant has concomitant thrush. Specific treatment includes clotrimazole, myconazole, or nystatin. Mycolog contains potent fluorinated steroid and should be avoided
A relatively common disorder of unknown etiology that is seen in children and adolescents (40% of cases occurring in patients under 15 years of age), granuloma annulare is manifested by skin-colored papules which spread annularly with central involution to form 1-5 cm rings. Females are affected twice as frequently as males; the rash is most commonly noted on the hands and feet. This rash will resolve spontaneously in several months to several years (73% will disappear spontaneously within two years), so not providing treatment is an option. Recurrences are seen in up to 40% of patients at the original site. This disorder can be distinguished from dermatophyte infections because of the absence of scaling.

Kawasaki disease105 is an acute multi-system illness of unknown cause that was described in Japan in 1967. Though the etiology remains elusive, putative etiologic agents have included spirochetes, rickettsia, retroviruses, rug shampoo, and bacterial super-antigens. The median age of patients is two years, with 80% of affected children being less than five years of age. The diagnosis of Kawasaki disease rests on the identification of clinical criteria that fulfill the case definition and comparison of these features with the case definition criteria for toxic shock syndrome (TSS). The diagnosis is made by an abrupt onset of fever greater than 39.4°C for at least five days that is unresponsive to antipyretics and the presence of no other confounding infectious illness (seen in 95% of cases), plus four of the following five criteria (or three of the five criteria and the presence of coronary artery aneurysms on echo (atypical Kawasaki).
Fortunately, there are some major distinguishing features which help separate Kawasaki disease from toxic shock syndrome. KD is virtually limited to children under 10 years of age whereas TSS is primarily a disease of menstruating females. The presence of hypotension would strongly favor TSS. The duration of fever is typically shorter in TSS, lasting less than five days. The edema of the extremities in KD is more impressive than that seen in TSS and lasts considerably longer. The exanthem of KD appears as a truncal eruption which may be morbiliform (erythematous macules resembling measles or scarlatina). An early scarlatiniform perineal eruption is characteristic and progresses to desquamation more rapidly than the peeling on the finger tips seen at two to three weeks after the onset of the illness. Lymphadenopathy was once considered a hallmark of KD, hence the name "mucocutaneous lymph node syndrome," but this finding has proven to be the least reliable of the six criteria in the list above. The associated vasculitis of Kawasaki disease results in coronary artery abnormalities in up to 20% of patients (with up to 2% mortality), representing the determinant of long-term morbidity and mortality. Management of this disorder includes intravenous gamma globulin in conjunction with aspirin to reduce the risk of coronary artery complications. A meta-analysis of IVIG106-110 verses placebo showed a significant decrease in coronary artery abnormalities (CAA) in favor of IVIG at 30 days (RR is 0.74 with 95% CI 0.61 to 0.90). Furthermore, there was a trend toward benefit of IVIG at 60 days (p=0.06). The metaanalysis of 400 mg/kg/day for five days versus 2 grams/kg in a single dose showed a statistically significant reduction in CAA, the number of hospital days, the total medical expense, and fever at 30 days (RR is 4.47 with 95% CI 1.55 to 12.86).
Scabies is a contagious infestation of the skin caused by the mite Sarcoptes scabiei. It is estimated that at least 300 million people are infested with scabies worldwide. Clinically, it is an extremely pruritic eruption of papules and vesicles and, classically, burrows. The pathognomonic scabies burrow is an elevated serpiginous tract that measures up to 10 mm in length, occurs in only 10% of patients, and is frequently distorted by vigorous scratching. Burrows can be identified by a procedure that was published by Woodley.111 Fountain pen ink is applied to the suspected area of skin, then the surface ink is washed away. The tracts are outlined by the ink that trickled into the opening made by the burrowing mite. Older children usually have intertriginous, flexural area, belt-line, and perineal involvement. In younger children, lesions are more typically found on the palms and soles and the head and neck region. Diagnosis may be made by the combination of a history of persistent itching and clinical history of similar complaints in any close contacts. Secondary bacterial infections commonly complicate scabies and since scabies may be a sexually transmitted disease, adolescents with this illness should be evaluated for other STDs (gonorrhea and chlamydia). Diagnosis can be confirmed by scraping the involved skin (preferably burrows and fresh papules) and examining the material under low power for evidence of mites, eggs, or feces. The illness is treated with topical preparations, such as lindane and permethrin cream (Elimite). It is crucial that any scabies treatment be applied to the whole body, with special attention to the hand and feet and intertriginous areas. The scalp and face must be treated in children, with particular attention given to the post-auricular area. Many providers prefer permethrin112 (adverse reactions occur in 2.5% of those treated with this agent, most typically pruritis), since a study done with rats showed that lindane is 40 times more neurotoxic.113 Taplin114 found significantly higher cure rates among those treated with a single application of permethrin 5% cream (91%) than with lindane 1% (65%). Although cases of lindane tolerant scabies have been reported in the United States, a large multi-center trial by Schultz115 and coworkers demonstrated that 5% permethrin and 1% lindane had comparable efficacy for the eradication of this infestation (91% vs. 86%, respectively). Persistent pruritis was half as common with permethrin (14% vs. 25%). Although 5% permethrin is more expensive than lindane, its comparable efficacy and higher therapeutic index would make permethrin the preferred drug for the treatment of scabies in infants, where concern of systemic absorption of lindane and possible neurotoxicity due to product misuse are greatest. All household contacts, except pregnant women and infants, should be treated and all clothing and bed linens that have been used in the preceding two days should be washed in hot water. Though symptoms generally resolve within a few weeks of treatment, it is important to recognize that pruritis may persist for several weeks, even after effective therapy, which is due to a hypersensitivity reaction to the mite. Twenty four hours after treatment, the patient is no longer capable of transmitting the disease.
P. Capitis infestations are caused by Pediculosis humanus ; this louse commonly infests preschool and elementary school children and is commonly spread by sharing infested grooming items, having close contact with an infected person, or sharing clothing. Head lice can be found in any population, although it appears less common in African Americans since the insect seems poorly adapted to thick curly hair. Reports of increased rates of infestation in longhaired lower socioeconomic groups have not been confirmed. P. capitis is the most common form of lice, and pruritis of the scalp is a prime complaint. On examination, nits (lice ova) can be seen as tiny white oval bodies firmly attached to the hair shaft which fluoresce a pearly white color under Wood's light. If identification is in doubt, the hair may be studied under a microscope for clarification. The clinician may differentiate nits from dandruff by the fact that the latter pull off the hair shaft easily.

P. pubis, caused by Phthirus pubis (crab louse), is quite different in appearance from the body louse; it has a short crab-like body and an anterior pair of legs with delicate hooks. It is also associated with intense pruritis, and the nits are found on the pubic hairs. This infestation is particularly common during adolescence since it is a sexually transmitted disease; up to 50% of patients with P. pubis will have another STD. P pubis prefers the pubic area, but this lice can infest other short-haired regions, such as the axillae, facial hair, and eyelashes (especially in children). Eyelid infestation may be a marker of child abuse.
As in scabies, lindane and permethrin112-115 cream are the treatment options (the latter preferred for the reason noted previously). An increasing rate of resistance to over the counter preparations, such as pyrethrin (RID) and permethrin 1% (Nix), has been observed; at which time, permethrin 5% cream is recommended once weekly for two weeks. P. pubis and capitis should be treated with two applications of pediculocide one week apart because the incubation period of louse ova is 6 to 10 days. In several studies, Taplin114 noted that permethrin has proven to be significantly more effective than lindane for the eradication of P. capitis. These investigations found failure rates at two weeks post-treatment to be 1-3% for permethrin and 15-57% for 1% lindane shampoo. Advantages offered by permethrin include a long half-life, which provides protection against re-infestation. All family members/sexual partners should be examined and the school should be notified when a confirmed case is identified. Nits can be removed with a fine tooth comb. P. pubis infestation of the eyelashes is best treated with the application of petrolatum (physostigmine is an alternative) two to four times daily to the lashes to asphyxiate the lice and nits. Lastly, antihistamines may be prescribed for the short term symptomatic relief of pruritis.
Lyme disease48-90,118-119 is caused by bites of ixodid ticks infected with Borrelia burgdorferi. It was first reported by Steere118 in 1977 and named after the community of Lyme, Connecticut where the initial cases were clustered. An individual is at greatest risk of infection when a tick has been attached to the skin for more than 24 hours. The peak incidence is during the summer and early fall and the illness presents in three stages:
In early Lyme disease, most patients have an elevated IgM to the spirochete which peaks at six weeks after onset of illness. The enzyme-linked immunoabsorbent assay (ELISA) has been reported to be 50% sensitive in early disease and 85% sensitive one month after the onset of illness. Therefore, early LD remains a clinical diagnosis based upon a typical EM rash; negative serology should not exclude this consideration. Culture of a spirochete is rarely helpful. Antibiotics should be commenced once the diagnosis is suspected to prevent later complications. In children under eight years of age, the suggested treatment is penicillin V 50 mg/kg/day (although it is slightly less effective than tetracycline, which is recommended for adults) or erythromycin 30 mg/kg/day (for patients with penicillin alergy) for two to three weeks. Permethrin112,119 applied to clothing is the most effective tick repellent. Other measures to help prevent tick bites include wearing light colored clothing for easy identification of crawling ticks, regularly checking the body and pets for ticks, wearing protective garments, and removing attached ticks promptly with tweezers.119
Insect bites are common in children, with mosquitos and fleas being the most common perpetrators. Papules, urticarial wheals, lesions which manifest within minutes of the bite, vesicles, and bullae are not uncommon. Clues to the correct diagnosis include consideration of the season, geographic area, presence of pets, distribution, and central punctum. Mosquito bites are generally limited to spring and summer; flea bites occur year-round and are usually associated with contact with dogs and cats. Lesions are noted on exposed surfaces of the extremities, head, and face. Fleas may survive for several months in carpeting or upholstery without a meal, thus, it is important to consider Lyme disease in a patient who recently moved into a home where a pet once lived. Unlike mosquitos, a linear grouping of flea bites is common, reflecting an insect's progressive feeding (breakfast, lunch, and dinner). Many other insects, including bees and wasps, affect children and it is not within the scope of this paper to discuss them all. Localized reactions to these bites and stings are treated symptomatically. Treatment is limited to antihistamines and prevention of bites with repellents, home extermination, and treatment of pets with insecticides. There has been recognition over the past decade of the neurotoxic effects of diethyltoluamide (DEET),120-131 though considering billions of past users, DEET has a good safety profile after 50 years of worldwide use. In comparison trials, DEET is more effective than any other insect repellent. The appropriate and safest concentration to use on children remains unclear. Due to potential absorption through the skin, prudence would dictate that the lowest effective concentration be used. When DEET based repellents are applied in combination with permethrin treated clothing, protection against insect bites of nearly 100% can be achieved. Ultrasonic devices and bug "zappers" are ineffective against mosquitos.
A skin eruption while the child is taking a medication should be considered a potential drug reaction. Sulfonamides are responsible for the majority of reactions. Hospitalized patients are more likely (30%) to develop a reaction to a drug because of multiple exposures, with up to 3% of admitted children developing a reaction. Arndt et al131 showed that reactions occurred at a rate of 59 per 1000 drug courses of trimethoprim-sulfamethoxazole, while the use of chloral hydrate was associated with 0.2 reactions per 1000 courses. Penicillin causes reactions at a rate of 3 per 1000 courses of therapy; it affects up to 10% of the adult population, with fatal anaphylaxis occurring in 2 of 100,000 adult patients. The appearance of drug reactions is nonspecific and may mimic any dermatosis, although certain patterns should make the clinician suspicious. Eosinophilia, thought to occur commonly with drug reactions, is actually uncommon. The important hypersensitivity disorders are urticaria, erythema nodosum, and erythema multiforme.
Urticaria occurs at some time in the life of 20% of the population and in 3% of all children. Lesions present acutely and are transient in nature (individual lesions resolve within 24 hours). The etiology remains unclear in the majority of cases. When lesions last longer than 24 hours, consider an alternative diagnoses, such as erythema multiforme. Urticaria appears as well demarcated wheals that are intensely pruritic, appear suddenly, last up to a few hours, resolve, and reappear in another location. Angioedema is a term used to describe non-pruritic swelling of the eyelids, hands, lips, and tongue and it often shares a common etiology with urticaria. Lesions secondary to physical agents generally are concentrated in those areas of direct stimulation (dermatographism). The respiratory, cardiovascular, and gastrointestinal systems may be involved, resulting in potentially life-threatening reactions. Symptoms may include stridor, dyspnea, wheezing (from laryngospasm/ bronchospasm), as well as hypotension, nausea, and vomiting and diarrhea. Urticaria usually is acute and transient, but if it persists longer than six weeks, it is called chronic urticaria. Although chronic urticaria sometimes is associated with physical agents or systemic disease (viral hepatitis, juvenile rheumatoid arthritis, SLE, lymphoma, etc), the etiology remains unknown in more than 90% of pediatric cases. Laboratory tests are generally unrewarding in acute urticaria; though, as depicted in the algorithm (Clinical Pathway: Urticaria), there are tests (CBC, ESR, monospot, ANA, liver function tests, stool for ova and parasites, etc) that can assist in the work-up. Possible causes of uticaria are listed in Table 1.

Symptomatic treatment includes antihistamines and elimination of identified etiologic factors, whenever possible. The subcutaneous administration of 1:1000 epinephrine is beneficial in children with angioedema and severe urticaria. Steroids should be reserved for those patients unresponsive to the modes of therapy referred to above. A prospective double-blinded controlled trial132 looking at 25 patients with urticaria compared 20 mg famotidine (H2 antagonist) with 50 mg diphenhydramine (H1 antagonist). Thirty minutes prior to and after treatment, patients rated pruritis and sedation using a visual analogue scale, while physicians evaluated intensity of urticaria. Famotidine132 was found to reduce pruritis and intensity of urticaria without causing sedation. Famotidine was comparable to diphenhydramine in efficacy; however, there was a non-significant trend for the latter medication to be more effective in the treatment of pruritis. Another study133 of 93 emergency department patients with urticaria comparing 300 mg cimetidine and 50 mg diphenhydramine showed that each medication provided significant relief of itching and wheal intensity (p less than 0.0001). Sedation was caused by both diphenhydramine (p less than 0.0001), and cimetidine (p less than 0.0006); however, the degree of sedation caused by the former medication was significantly greater than that caused by cimetidine (p less than 0.0001). The perception of overall improvement was greater with cimetidine (87%), whereas 76% reported improvement with diphenhydramine. Finally, a study by Foulds134 et al comparing cimetidine and promethazine singly and in combination revealed no significant clinical difference.

Erythema nodosum may be seen in adolescents and appears as deep tender erythematous nodules 1-5 cm in diameter on the pretibial surfaces of the legs. The eruption usually lasts three to six weeks. Though the immunologic mechanism has not been clarified, potential etiologies include: strep pharyngitis, TB, inflammatory bowel disease, malignancies, and, rarely, drugs (sulfonamides, dilantin, and oral contraceptives). Treatment is directed at the cause of the disorder and elevation of the legs helps to reduce pain and swelling. Analgesics are helpful.
Erythema multiforme135-138 is an acute hypersensitivity reaction which presents in two distinct forms: (1) EM minor, characterized by symmetrical erythematous macules or wheals with superimposed vesicles primarily involving the extensor surface of the arms, legs, trunk, palms, and soles that evolve into annular "target" lesions, and (2) EM major, or Steven-Johnson syndrome, characterized by bullae/ulceration's of at least two mucosal surfaces (lips, conjunctivae, nasal/oral/vaginal mucosa) accompanying typical cutaneous EM lesions. Systemic manifestations of EM minor are mild and consist of low grade fever, malaise, and myalgia. This is in contrast to EM major which is associated with an acute high fever, cough, sore throat, vomiting and diarrhea, and arthralgias. When the eyes are involved in EM major, blindness has been described in up to 10% and mortality remains at approximately 10%. In a study by Huff et al136 of recurrent EM, all patients studied had a history of recurrent herpes (often of the lip), on average, 9.5 days before the onset of an episode of EM. Lesions of EM from all patients studied show evidence of HSV antigen by immunofluorescence. Furthermore, a study looking at treating HSV infection in adults with oral acyclovir showed that it can significantly reduce outbreaks of EM, though there is no utility of anti-viral therapy in established EM. Werchniak et al137 and Cohen et al138 presented seven case reports of EM complicating severe Rhus allergic contact dermatitis. Other precipitants of EM include mycoplasma pneumoniae and drugs (sulfonamides, penicillins, hydantoins, carbamazepine,141 and barbiturates). EM minor is self limited, usually evolving over two weeks, with complete healing by a month.
The management of EM in children is controversial.139 Clearly, any instigating agent, such as a drug or infection, should be eliminated/treated. EM minor lesions may be treated conservatively with the application of cool compresses and antihistamines. Painful oral mucosal lesions may derive benefit from BMX (benadryl/maalox/viscous (xylocaine)), though the toxic profile of the latter ingredient must be considered. Kakourou et al143 evaluated the effectiveness of systemic steroids in EM major in a prospective study of 16 children; 10 children received 4 mg/kg/day of methylprednisolone and six children served as controls. Their study showed:
The use of steroids for EM (minor or major) is a complicated issue, with few convincing studies to guide usage.142-145 In fact, many studies argue that steroid use is of no value and may increase morbidity from bleeding and sepsis as well as increase the length of hospital stay. However, all studies have been retrospective, unmatched, and largely in-hospital based perhaps biasing steroid use to those patients who were sicker. Steven-Johnson syndrome with more than 30% skin denudation should be managed in a burn unit or intensive care unit. Treatment includes meticulous skin care and fluid and electrolyte management.
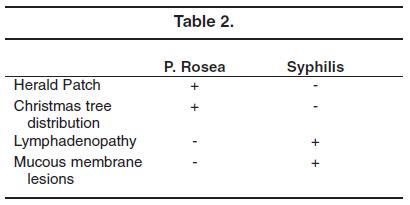
This very common eruption, typically seen in children over 10 years of age, presents acutely with mildly pruritic erythematous oval patches with a collarette of scale, classically in a Christmas tree distribution on the trunk (turtle neck sweater distribution). The herald patch, which typically occurs on the trunk, neck, or proximal arms, precedes the eruption in approximately 80% of cases by about one week and is similar to the acute eruption but is usually larger. The herald patch may be mistaken for tinea corporis, but a KOH preparation eliminates this possibility. Pityriasis is thought to be caused by a virus, though none has been isolated to date. It usually resolves within two months and treatment is symptomatic, with antihistamines and topical antipruritics. Secondary syphilis, another papulosguamous eruption, must be considered in sexually active adolescents.

Molluscum contagiosum is a common childhood contagious viral infection of the skin and is caused by a poxvirus. It is more frequently seen in swimmers and wrestlers; those affected by atopic dermatitis and immunosuppression are especially susceptible. The face, chest, and upper extremities are most commonly involved. Clinically, there are discrete skin-colored dome shaped 2-5 mm umbilicated papules alone or in groups, which may have an erythematous base. They are usually asymptomatic. Most lesions resolve spontaneously in under a year. Treatment of a single lesion includes the removal of the core with a comedone extractor/sterile needle or application of liquid nitrogen 0.7% or cantharidin. Multiple lesions are treated with the application of 0.1% retinoic acid.

Warts affect up to 10% of the population and are caused by the human papilloma virus (HPV), including verruca vulgaris (common wart), verruca plana (flat wart), verruca plantaris (plantar wart), and condylomata accuminata (genital warts). The incubation period lasts up to six months. Seen most commonly during adolescence, verrucous lesions begin as pinpoint skin-colored papules which evolve into a papilloma (resembling cauliflower). Most are not painful, though plantar warts may be an exception. Genital warts can be sexually transmitted and thus, in children, the possibility of abuse must be considered.147-152 Since perinatal transmission is possible, children younger than three years of age may have acquired the infection by this route. Innocent transmission of common warts may occur via infected caregivers during bathing and changing diapers. Cohen et al 146 performed a clinical study of condylomata acuminata in 73 pre-pubertal children (75% were younger than three years of age), evaluating for possible sexual abuse. None were found to be abused. Seven children had warts that were of the same serotype of lesions found in the mother. In another study, Obalek et al153 found that condylomata were found in 22 mothers of 32 children with genital warts; those children did not develop lesions until a mean age of 2 years 10 months, arguing for a long latency. Interestingly, seven children with condylomata of three mothers with hand warts were found to have identical viral serotypes. Dejong et al154 described 40 children with condylomata; sexual abuse was not found in 14 children under three years of age. Padel et al155 presented 17 children with condylomata; one of seven under age three years was abused. It appears that there is frequent nonsexual transmission of HPV in young children.
Warts may take years to resolve without treatment (25% disappear spontaneously within six months and 65% disappear spontaneously within two years). Several courses of treatment will be necessary since treatment failure is not uncommon (10%). Common treatment modalities rely on the destruction of the infected tissue and include keratolytics (salicylic acid/lactic acid), blistering agent (0.7% cantharidin), and cryotherapy with liquid nitrogen. Salicylic acid is the least painful method of treatment, although resolution may take longer than with cryotherapy. A simple painless method of periungual wart removal was reported by Litt.156 With this technique, the involved finger is enshrouded in common adhesive tape. The tape is removed for 12 hours every week and then reapplied. The wart generally disappears within a month. Oral cimetidine has been reported to be useful in the treatment of warts, though other studies refute this.117
Congenital Melanocytic nevi116,157,163-166 are noted in 1% of newborns. Congenital nevi are small (most less than 3 cm), symmetrical, uniform in color (brown), and have smooth borders. When examining moles, it is important to keep in mind the ABCD's of melanoma (suspicious mole that has been changing, bleeding or ulcerating - Asymmetry, irregular Border, varying Color, Diameter greater than 6 mm). The biologic course of congenital melanocytic nevi is fairly stable, with lesion growth proportionate to somatic growth. The most commonly used classification of nevi designates small congenital melanocytic nevi to be less than 1.5 cm, intermediate lesions 1.5 cm to 20 cm, and giant congenital melanocytic nevi greater than 20 cm.

Controversy exists as to the management of giant congenital nevi since, based upon a series of 151 patients with a mean age of eight years,157 the lifetime risk for the development of melanoma is 4.7%. Another study by Rhodes et al163,164 estimated this risk to be 6.3%, based on a series of 39 patients followed for 8.6 years. A third study by Quaba and Wallace158 calculated a melanoma risk of 8.5% during the first 15 years of life. The incidence of giant congenital melanocytic nevi is 1 in 1160 (series involving 4641 newborns in the U.S.) to 1 in 20,500 (series involving 532,831 newborns in the South America), but they account for one third of pre-pubertal melanomas, suggesting that children with this lesion have a 17-fold relative risk as compared to the general population. There are several reasons for the wide range of reported risk of congenital nevi: the studies sited are retrospective, reports are from referral centers whose population may be biased to more complicated nevi, and there are differences in the definition of giant nevi used by the authors. Melanomas may arise in GCN early in life, with 40-70% occurring before puberty; however, only 2% of melanomas occur in patients younger than 20 years of age and up to 80% develop without predisposing nevi. In children with nevi overlying the mid-line spine, it is necessary to evaluate the patient for underlying abnormalities of bone and CNS. Many physicians argue that lesions accessible to examination may be observed serially for changes, with referral to dermatology for possible biopsy when worrisome changes occur. It is unknown how effective this method is in reducing the incidence of melanoma arising in giant nevi.157,164-166
Small congenital nevi are 10 times more common than their giant cousins. The risk of melanoma in adults with small nevi was estimated by Rhodes and Melski163 to be 21 times that of the unaffected population, though these studies suffer from similar methodologic issues noted previously. It is usually after adolescence that these lesions undergo malignant transformation, with a risk of approximately 5% for small congenital nevi in patients who live to the age of 60 years.
Dysplastic nevi differ from common nevi by their larger size (5-10 mm), presence on the trunk and buttocks, and their continued development throughout life. Lesions are macular, manifest variegated in color (tan/brown/pink), and have an irregular border. Effectiveness of serial surveillance for early detection of melanoma has been demonstrated.
The incidence of melanoma in the United States is increasing:162 in 1935 - incidence was 1 in 1500, 1989 - incidence was 1 in 128, and 2000 - incidence was 1 in 90. Fortunately, these tumors rarely occur in pediatric patients (incidence is 0.1/100,000 among children younger than age nine years, 0.2/100,000 in 10 through 14 year olds, and 1.4/100,000 in 15 through 19 year olds). Epidemiologic data from a variety of sources support a role for sunlight exposure in the causation of melanoma.167-169 Several studies have demonstrated an inverse relationship between the latitude at which one resides and the risk of developing melanoma. In a study of European borne immigrants to Israel, Anaise et al167 found the incidence of melanoma to be substantially higher among those who had resided in Israel for 20 to 30 years (58/million) than among those who had lived in the country for only two to five years (17/million). Recent investigations suggest that sun exposure during the first 10 to 15 years of life is a particularly important determinant of developing melanoma. A study by Sober et al168 demonstrated that, when compared to control subjects, patients with melanoma were twice as likely to have suffered a blistering sunburn during adolescence and 2.5 times as likely to have spent extended vacations (more than 30 days) in sunny places as a child. Mackie et al169 found that the number of nevi present was the most important of the melanoma risk factors investigated, with freckling and sunburn being less powerful predictors. Holly et al165 found similar risk rates, see Table 3.

As in adults, the prognosis of melanoma in children depends on the depth of invasion of the lesion. Skov-Jensen et al161 reviewed the literature on melanoma in children and calculated that the three year survival rate with regional lymph node metastases approximated the expected five year survival rates in adults. They proposed that the poorer prognosis was caused by delayed diagnosis. In a series of 25 patients younger than 20 years of age, a delay in diagnosis ranging from a few months to five years occurred in 60%, most often as a result of failure of a physician to recognize the malignant nature of the lesion. Therapy for melanoma in children is extrapolated from adult experience and is primarily surgical. Meta-analyses by Dennis et al170 and Huncharek et al171 called into question the association between melanoma and sunscreen use, yielding a RR of 1.01, indicating no association.

Pediatric dermatology often poses a challenge to practitioners of emergency medicine. When making dermatologic diagnoses, it is important to examine the skin carefully, paying special attention to distribution of lesions, morphology, and hair, nail, and mucosal changes. Children often present to the emergency department with rashes ranging from the mundane (insect bites and poison ivy) to the downright challenging (Kawasaki and Steven-Johnson syndrome). When confronted by a child with an enigmatic rash, the clinician should develop a list of differential possibilities, a plan of how to address each of these possibilities, and, finally, a management plan recognizing some of the controversies that may exist in that plan. The clinician has access to many of the tools that can aid in making the correct diagnosis (e.g., a clinical laboratory, a microscope, and a wood's lamp) and there are numerous reference texts that may help the emergency physician in this endeavor.
After the attending physician discussed the case with a resident, it was decided that the child met criteria for the diagnosis of Kawasaki disease based on the following facts: the child is three years old, had a temperature of 40 for eight days that was unresponsive to typical doses of antipyretics, had bilateral conjunctivis, manifested a non pruritic generalized truncal rash, had swollen hands and feet, had no clearly defined other etiology for the fever (blood cultures were negative), and manifested "paradoxical irritability."
The child was admitted to the inpatient service where IV gamma globulin and aspirin were started. Two weeks after initial presentation, he had a coronary ultrasound which did not reveal evidence for an aneurysm. The cardiologist recommended a repeat study in three months.

|
|
 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Evidence-based medicine requires a critical appraisal of the literature based upon study methodology and number of subjects. Not all references are equally robust. The findings of a large, prospective, randomized, and blinded trial should carry more weight than a case report.
To help the reader judge the strength of each reference, pertinent information about the study, such as the type of study and the number of patients in the study, will be included in bold type following the reference, where available.
Marc S. Lampell
April 1, 2007
Pediatric Emergency Medicine Practice • CONTINUE READING
Access every issue, our complete clinical pathway library, and earn up to 190 CME credits with an annual subscription.
Stay current with a new Pediatric Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933