
|
|
Although the incidence of pediatric venous thromboembolism is increasing, it is often overlooked in children due to the overall low incidence. This issue reviews the epidemiology of pediatric venous thromboembolism, including the factors that have led to its increasing prevalence, and discusses the physiology of hemostasis and coagulation. Key features of the history and physical examination, as well as identification of risk factors, are reviewed, as these have the most diagnostic value for venous thromboembolism in pediatric patients. Recommendations are also provided for diagnostic testing and management in the emergency department.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
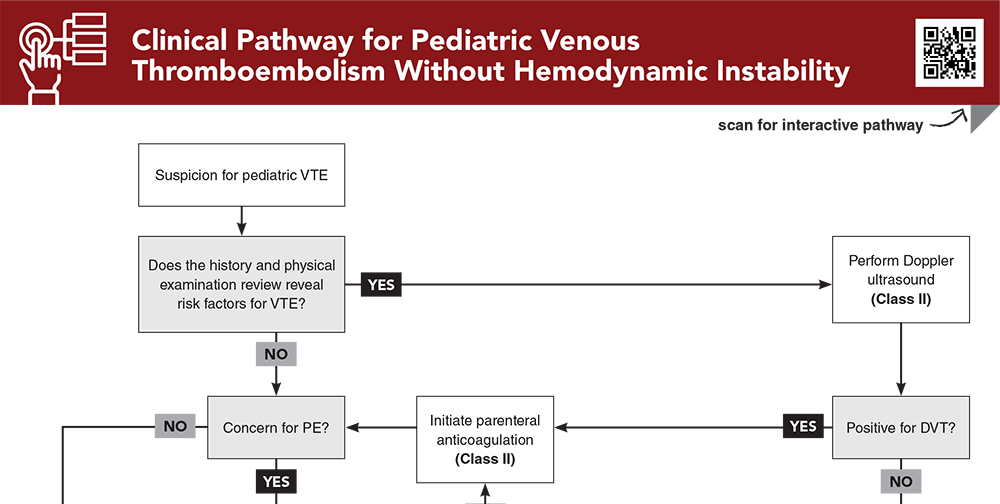
Subscribe to access the complete flowchart to guide your clinical decision making.
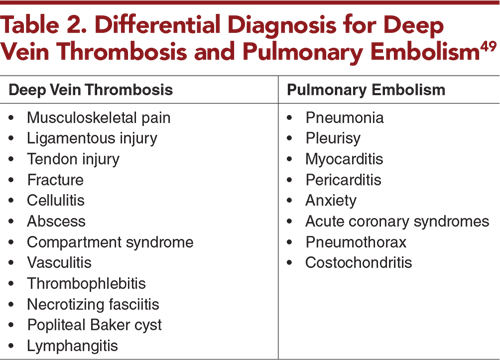
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
4. * Monagle P, Chan AKC, Goldenberg NA, et al. Antithrombotic therapy in neonates and children: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e737S-e801S. (Practice guidelines) DOI: 10.1378/chest.11-2308
5. * Monagle P, Cuello CA, Augustine C, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: treatment of pediatric venous thromboembolism. Blood Adv. 2018;2(22):3292-3316. (Society guidelines) DOI: 10.1182/bloodadvances.2018024786
69. * Hennelly KE, Baskin MN, Monuteuax MC, et al. Detection of pulmonary embolism in high-risk children. J Pediatr. 2016;178:214-218. (Retrospective; 561 patients) DOI: 10.1016/j.jpeds.2016.07.046
86. * Male C, Lensing AWA, Palumbo JS, et al. Rivaroxaban compared with standard anticoagulants for the treatment of acute venous thromboembolism in children: a randomised, controlled, phase 3 trial. Lancet Haematol. 2020;7(1):e18-e27. (Multicenter, parallel-group, open-label, randomized study; 520 patients) DOI: 10.1016/S2352-3026(19)30219-4
87. * Goldenberg NA, Kittelson JM, Abshire TC, et al. Effect of anticoagulant therapy for 6 weeks vs 3 months on recurrence and bleeding events in patients younger than 21 years of age with provoked venous thromboembolism: the Kids-DOTT randomized clinical trial. JAMA. 2022;327(2):129-137. (Randomized controlled trial; 417 patients) DOI: 10.1001/jama.2021.23182
98. * Halton J, Brandao LR, Luciani M, et al. Dabigatran etexilate for the treatment of acute venous thromboembolism in children (DIVERSITY): a randomised, controlled, open-label, phase 2b/3, non-inferiority trial. Lancet Haematol. 2021;8(1):e22-e33. (Randomized controlled trial; 267 patients) DOI: 10.1016/S2352-3026(20)30368-9
Subscribe to get the full list of 122 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: deep vein thrombosis, DVT, venous thromboembolism, VTE, pulmonary embolism, PE, thrombus, D-dimer, Wells criteria, PERC rule, coagulation, anticoagulation, heparin, unfractionated heparin, UFH, low-molecular-weight heparin, LMWH, vitamin K antagonist, direct oral anticoagulant, DOAC, thrombolysis, central venous catheter, CVC, occluded central venous catheter, catheter occlusion, thrombophilia, hemodynamic instability, postthrombotic syndrome
Michael P. Johnson, MD; Asim A. Abbasi, MD, MPH
Nicole Gerber, MD; Tim Horeczko, MD, MSCR, FACEP, FAAP
May 1, 2024
May 1, 2027 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAP Prescribed Credits, 4 AOA Category 2-B Credits.
Pediatric Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Pediatric Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933