
|
|
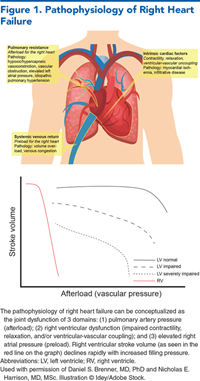
Right heart failure (RHF) can result from many cardiac, pulmonary, and systemic pathologies. Common causes of RHF include pulmonary embolism, left heart failure, congenital heart disease, chronic lung disease, acute myocardial infarction, infiltrative disease, infectious disease, and valvular abnormalities. Acute and chronic RHF confer a high risk for morbidity and mortality in the acute care setting, and interventions commonly used in emergency care can prompt acute decompensation if the RHF is not recognized. The severity of presentation may range from compensated clinically silent cardiovascular dysfunction to venous congestion, multiorgan failure, and circulatory collapse. This review describes the pathophysiology of right heart failure and offers an evidence-based approach to the diagnosis, management, and disposition of both acute and chronic RHF.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
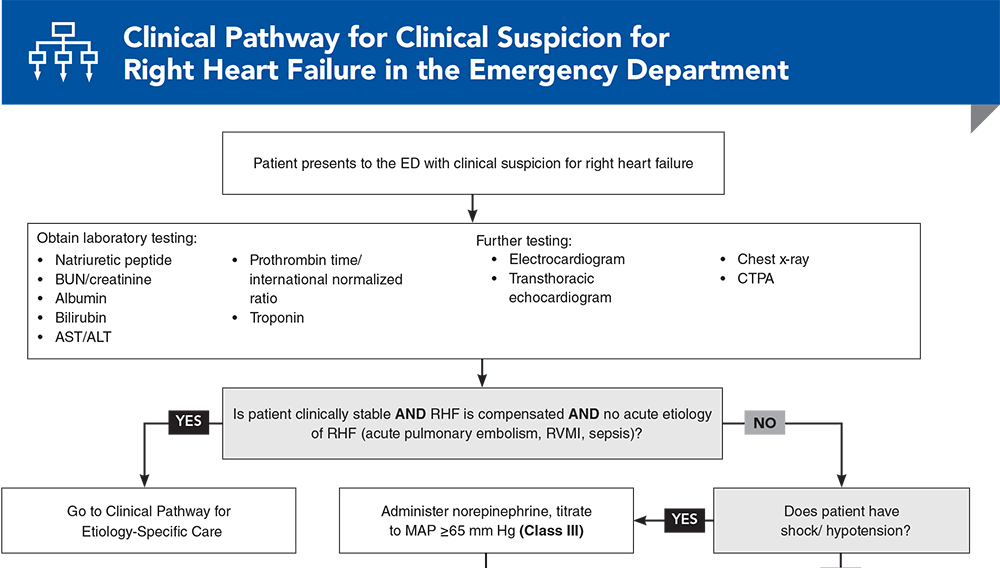
Subscribe to access the complete flowchart to guide your clinical decision making.
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
1. * Konstam MA, Kiernan MS, Bernstein D, et al. Evaluation and management of right-sided heart failure: a scientific statement from the American Heart Association. Circulation. 2018;137(20):e578-e622. (Guideline) DOI: 10.1161/CIR.0000000000000560
* Harjola VP, Mebazaa A, Celutkiene J, et al. Contemporary management of acute right ventricular failure: a statement from the Heart Failure Association and the Working Group on Pulmonary Circulation and Right Ventricular Function of the European Society of Cardiology. Eur J Heart Fail. 2016;18(3):226-241. (Guideline) DOI: 10.1002/ejhf.478
21. * Gorter TM, Hoendermis ES, van Veldhuisen DJ, et al. Right ventricular dysfunction in heart failure with preserved ejection fraction: a systematic review and meta-analysis. Eur J Heart Fail. 2016;18(12):1472-1487. (Systematic review, meta-analysis; 4835 patients) DOI: 10.1002/ejhf.630
22. * Harrison NE, Ehrman R, Favot M, et al. Right ventricular dysfunction in acute heart failure from emergency department to discharge: predictors and clinical implications. Am J Emerg Med. 2022;52:25-33. (Prospective study; 84 patients) DOI: 10.1016/j.ajem.2021.11.024
24. * Judge P, Meckler G. Congenital heart disease in pediatric patients: recognizing the undiagnosed and managing complications in the emergency department. Pediatr Emerg Med Pract. 2016;13(5):1-28. (Review)
37. * Huang SJ, Nalos M, Smith L, et al. The use of echocardiographic indices in defining and assessing right ventricular systolic function in critical care research. Intensive Care Med. 2018;44(6):868-883. (Systematic review, meta-analysis; 81 studies) DOI: 10.1007/s00134-018-5211-z
38. * Harrison NE, Favot MJ, Gowland L, et al. Point-of-care echocardiography of the right heart improves acute heart failure risk stratification for low-risk patients: the Reed-AHF prospective study. Acad Emerg Med. 2022;29(11):1306-1319. (Prospective study; 120 patients) DOI: 10.1111/acem.14589
53. * Lim P, Delmas C, Sanchez O, et al. Diuretic vs. placebo in intermediate-risk acute pulmonary embolism: a randomized clinical trial. Eur Heart J Acute Cardiovasc Care. 2022;11(1):2-9. (Randomized controlled trial; 276 patients) DOI: 10.1093/ehjacc/zuab082
83. * Mekontso Dessap A, Boissier F, Charron C, et al. Acute cor pulmonale during protective ventilation for acute respiratory distress syndrome: prevalence, predictors, and clinical impact. Intensive Care Med. 2016;42(5):862-870. (Prospective study; 752 patients) DOI: 10.1007/s00134-015-4141-2
Subscribe to get the full list of 89 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
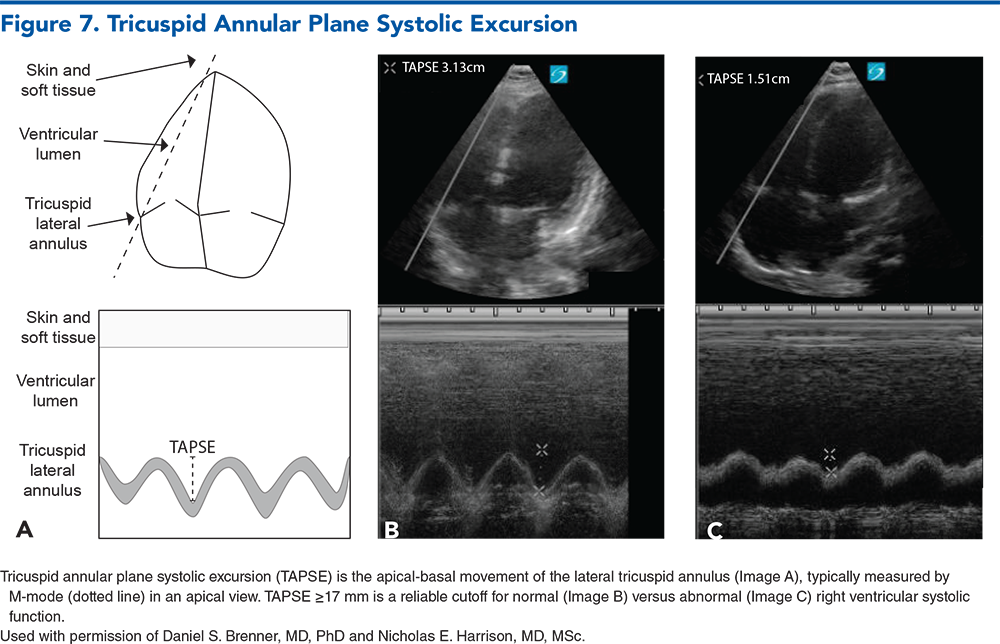
Keywords: right heart failure, pulmonary hypertension; myocardial infarction, TAPSE, pulmonary embolism, sepsis, acute respiratory distress syndrome, ARDS, congenital, TTE, ECMO
Daniel S. Brenner, MD, PhD; Onyedika J. Ilonze, MD; Shelby Beil, MD; Kellie Kaneshiro, AMLS; Nicholas E. Harrison, MD, MSc
James Morris, MD, MPH, FACEP; Kestrel Reopelle, MD, MEd
February 1, 2024
February 1, 2027 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933