

|
|
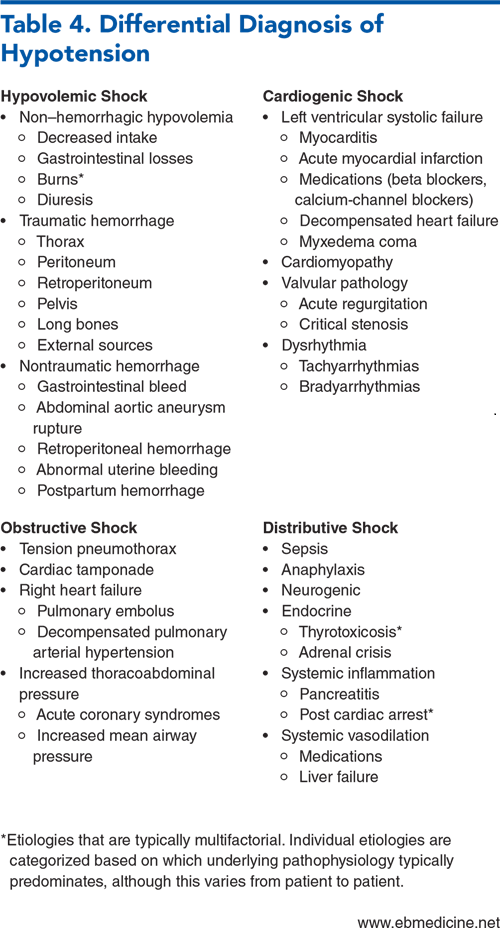
Hypotension can be a sign of significant underlying pathology, and if it is not rapidly identified and addressed, it can contribute to organ injury. Treatment of hypotension is best targeted at the underlying etiology, although this can be difficult to discern early in a patient’s disease course. Expedited bedside evaluation with rapid initiation of treatment based on the most likely underlying etiology is paramount, followed by serial reassessment of the patient’s condition. This review synthesizes the key aspects of the presentation and evaluation of a patient with hypotension, including salient historical features, physical examination findings, and diagnostic tests that can help guide treatment.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.

Subscribe to access the complete flowchart to guide your clinical decision making.

Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
2. * Holler JG, Bech CN, Henriksen DP, et al. Nontraumatic hypotension and shock in the emergency department and the prehospital setting, prevalence, etiology, and mortality: a systematic review. PLoS One. 2015;10(3):e0119331. (Systematic review) DOI: 10.1371/journal.pone.0119331
18. * Hernandez G, Ospina-Tascon GA, Damiani LP, et al. Effect of a resuscitation strategy targeting peripheral perfusion status vs serum lactate levels on 28-day mortality among patients with septic shock. JAMA. 2019;321(7):654-664. (Randomized controlled trial; 424 patients) DOI: 10.1001/jama.2019.0071
22. * Yoshida T, Yoshida T, Noma H, et al. Diagnostic accuracy of point-of-care ultrasound for shock: a systematic review and meta-analysis. Crit Care. 2023;27(1):200. (Meta-analysis; 12 studies, 1132 patients) DOI: 10.1186/s13054-023-04495-6
32. * Gordon AC, Mason AJ, Thirunavukkarasu N, et al. Effect of early vasopressin vs norepinephrine on kidney failure in patients with septic shock. JAMA. 2016;316(5):509-518. (Randomized controlled trial; 409 patients) DOI: 10.1001/jama.2016.10485
41. * Self WH, Semler MW, Wanderer JP, et al. Balanced crystalloids versus saline in noncritically ill adults. N Engl J Med. 2018;378(9):819-828. (Crossover trial; 13,347 patients) DOI: 10.1056/NEJMoa1711586
62. * Myburgh JA, Higgins A, Jovanovska A, et al. A comparison of epinephrine and norepinephrine in critically ill patients. Intensive Care Med. 2008;34(12):2226-2234. (Randomized controlled trial; 280 patients) DOI: 10.1007/s00134-008-1219-0
85. * Crowe E, DeSantis SM, Bonnette A, et al. Whole blood transfusion versus component therapy in trauma resuscitation: a systematic review and meta-analysis. J Am Coll Emerg Physicians Open. 2020;1(4):633-641. (Systematic review and meta-analysis; 12 studies, 8431 patients) DOI: 10.1002/emp2.12089
86. * de-Madaria E, Buxbaum JL, Maisonneuve P, et al. Aggressive or moderate fluid resuscitation in acute pancreatitis. N Engl J Med. 2022;387(11):989-1000. (Randomized controlled trial; 249 patients) DOI: 10.1056/NEJMoa2202884
94. * Reitz KM, Kennedy J, Li SR, et al. Association between time to source control in sepsis and 90-day mortality. JAMA Surg. 2022;157(9):817-826. (Retrospective; 4962 patients) DOI: 10.1001/jamasurg.2022.2761
Subscribe to get the full list of 96 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: hypotension, shock, end-organ, hypovolemic, distributive, obstructive, cardiogenic, hemorrhage, sepsis, ultrasound, RUSH, ECG, POCUS, vasopressor, inotrope
Nickolas Srica, MD; Clark I. Strunk, MD
Beulah Augustin, MD; Colin Pesyna, MD
December 1, 2023
December 1, 2026 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits. Specialty CME Credits: Included as part of the 4 credits, this CME activity is eligible for 1 Pharmacology CME credit, subject to your state and institutional approval.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933

