

|
|
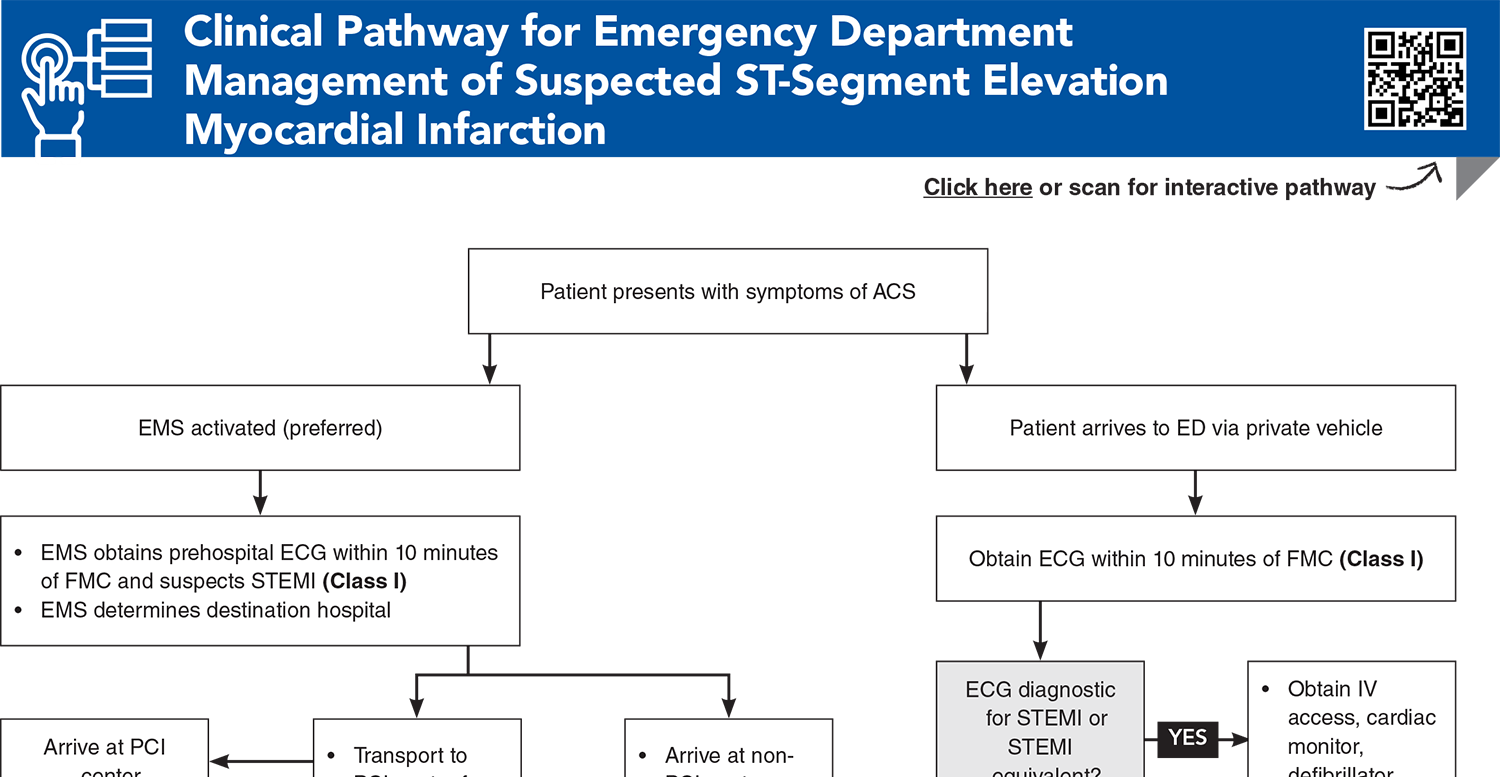
Acute coronary occlusion is a time-sensitive cardiac emergency that requires early, accurate diagnosis and prompt treatment to restore coronary perfusion, usually by percutaneous coronary intervention. Successful management of these patients demands a highly coordinated effort among emergency medical services, the emergency department, and cardiology. This issue highlights the importance of recognizing distinct electrocardiographic patterns that represent acute coronary occlusion, even in the absence of traditional STEMI criteria, and reviews evidence-based management recommendations.
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.
Subscribe to access the complete Clinical Pathway to guide your clinical decision making.
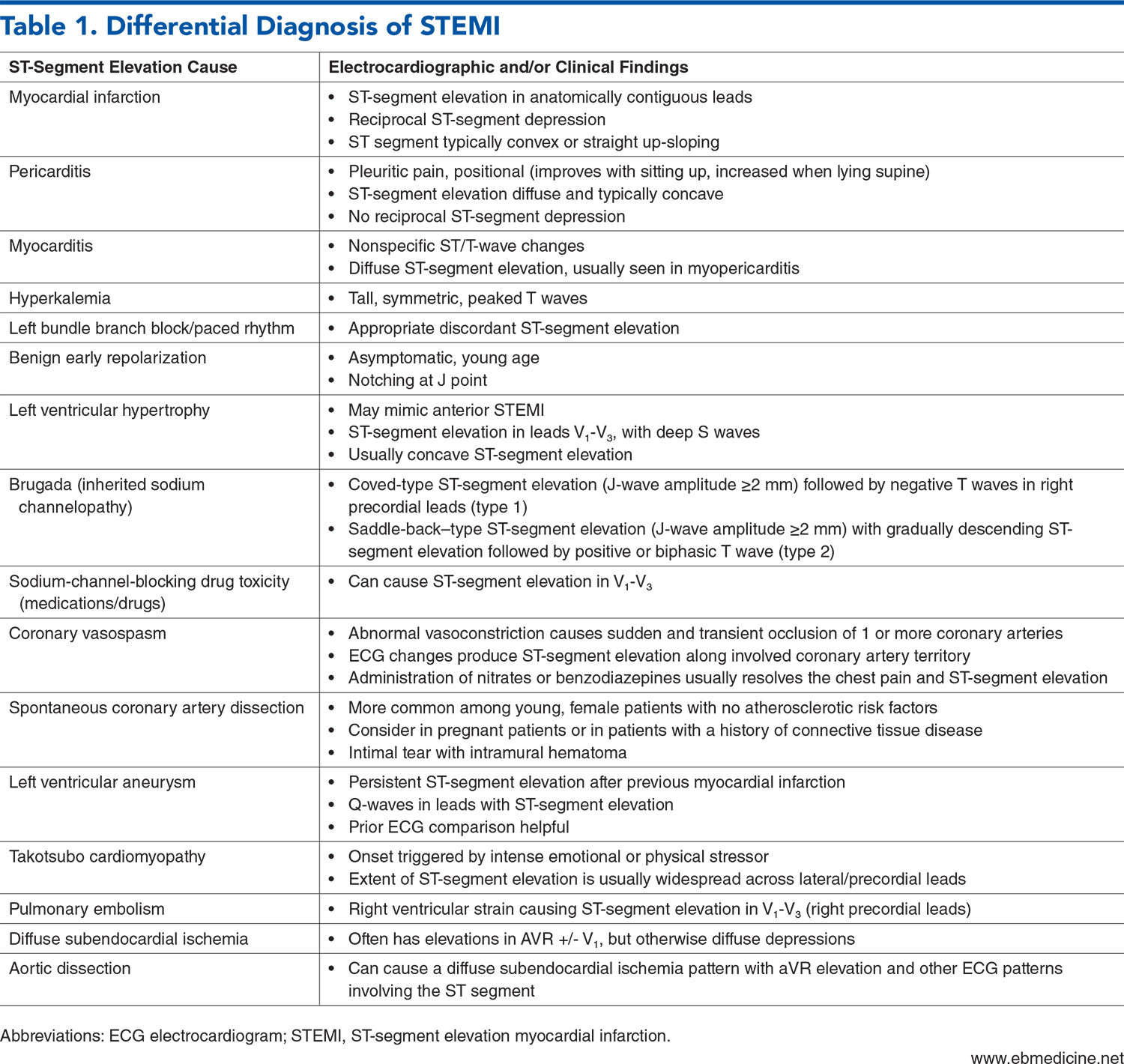
Subscribe for full access to all Tables and Figures.
Buy this issue and
Following are the most informative references cited in this paper, as determined by the authors.
1. * Writing Committee, Kontos MC, de Lemos JA, et al. 2022 ACC expert consensus decision pathway on the evaluation and disposition of acute chest pain in the emergency department: a report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2022;80(20):1925-1960. (Evidence-based practice guideline) DOI: 10.1016/j.jacc.2022.08.750
4. * O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):e362-e425. (ACC/AHA evidence-based practice guideline) DOI: 10.1016/j.jacc.2012.11.019
5. * Rao SV, O’Donoghue ML, Ruel M, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI guideline for the management of patients with acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2025;151(13):e771-e862. (ACC/AHA evidence-based practice guideline) DOI: 10.1161/CIR.0000000000001309
6. * Byrne RA, Rossello X, Coughlan JJ, et al. 2023 ESC guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44(38):3720-3826. (Evidence-based practice guideline) DOI: 10.1093/ehjacc/zuad107
20. * Smith SW, Dodd KW, Henry TD, et al. Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Ann Emerg Med. 2012;60(6):766-776. (Retrospective; 3 institutions, 162 patients) DOI: 10.1016/j.annemergmed.2012.07.119
Subscribe to get the full list of 66 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: ACO, STEMI, NSTEMI, ACS, ECG, OMI, PCI, myocardial infarction, equivalent, Sgarbossa, posterior, fibrinolytic, reperfusion
Jillian Horning, MD
Kestrel Reopelle, MD, PhD
February 1, 2026
February 1, 2029 CME Information
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-B Credits.
Emergency Medicine Practice • CONTINUE READING
Read this issue today — or unlock the entire library for a little more.
Stay current with a new Emergency Medicine Practice issue every month, plus unlimited access to our complete issue library, all Interactive Clinical Pathways, and up to 190 CME credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933
