Deep vein thrombosis (DVT) can present with a variety of nonspecific signs and symptoms, and can involve the upper or lower extremities. Management of patients with DVT has changed markedly over the last 10 years, moving from hospital admission for initiation of anticoagulation to outpatient management. Diagnosis requires a risk stratification process involving clinical decision rules, D-dimer testing, and ultrasonography. Once the diagnosis is confirmed, the patient should be engaged in shared decision-making regarding treatment options. Recurrent DVT, as well as managing DVT in pregnant women, the elderly population, and patients with malignancies are also discussed.
A 20-year-old woman presents with a 3-day history of left lower extremity pain and swelling. On examination, her left lower leg is visibly larger than the right. She is concerned that she has a “blood clot,” because her mother had one several years ago. She says that she does not have health insurance and will be self-paying for her visit. She asks you to keep the cost of the visit as low as possible. You wonder whether there is clinical decision rule that could be used to aid in choosing a cost-effective diagnostic strategy…
Your next patient is a 56-year-old man who is also complaining of left lower extremity pain and swelling. A venous duplex ultrasound confirms a deep vein thrombosis (DVT) in the popliteal vein. He notes that he is the primary breadwinner for his family and cannot stay in the hospital for treatment. He asks if there is any way he could be discharged to home with treatment. You recall that patients with an isolated DVT can be discharged home, but you cannot remember the protocol to initiate the discharge process…
Your last patient of the shift is a 76-year-old woman with right lower extremity pain and swelling. On examination, her right lower leg is swollen, but she has no discoloration or loss of pedal pulse. A venous duplex ultrasound confirms an extensive proximal DVT in the extremity. You anticoagulate the patient and call the internist for admission. The internist would like you to discuss the case with a vascular surgeon for possible thrombolysis. You wonder what the evidence is supporting thrombolysis in these patients…
How would you manage these patients? Subscribe for evidence-based best practices and to discover the outcomes.

Subscribe to access the complete flowchart to guide your clinical decision making.






Subscribe for full access to all Tables and Figures.
Following are the most informative references cited in this paper, as determined by the authors.
Subscribe to get the full list of 97 references and see how the authors distilled all of the evidence into a concise, clinically relevant, practical resource.
Keywords: deep vein thrombosis, DVT, distal, proximal, Factor V Leiden, prothrombin, cancer, malignancy, oral contraceptives, pregnancy, Paget-Schroetter, primary effort thrombosis, D-dimer, Wells score, ultrasound, venography, anticoagulation, heparin, low-molecular-weight heparin, LMWH, warfarin, direct oral anticoagulant, DOAC, direct thrombin inhibitor, Factor Xa, reversal, aspirin, stockings, IVC, thrombolysis, upper extremity
Price: $75
+4 Credits!
Topics:
Dr. Ashoo is a practicing emergency physician, board-certified in emergency medicine and clinical informatics. Join him as he takes you through the October 2020 issue of Emergency Medicine Practice: Management of Deep Vein Thrombosis in the Emergency Department
Get quick-hit summaries of hot topics in emergency medicine. EMplify summarizes evidence-based reviews in a monthly podcast. Highlights of the latest research published in EB Medicine's peer-reviewed journals educate and arm you for life in the ED.
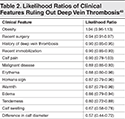
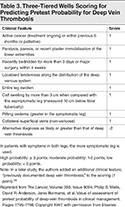
The Wells criteria for DVT are used to calculate risk of DVT based on clinical criteria.
The Wells criteria for deep vein thrombosis (DVT) stratifies patients suspected of having DVT into risk groups. The tool can be used in outpatient and emergency department settings.
Traditional testing for DVT involved costly and time-intensive multiple lower-extremity ultrasound. The Wells criteria can be used to determine which patients are overall unlikely to have DVT. Further testing with D-dimer can safely rule out DVT without the need for ultrasound. By risk-stratifying a patient to a low-risk category( Wells score < 2) and receiving a negative D-dimer, clinicians can eliminate the need for ultrasound to rule out DVT.
The Wells criteria stratify patients into “DVT unlikely” and “DVT likely” groups. An additional "moderate" risk group can be added, based on the sensitivity of the D-dimer being used. A score of ≤ 0 is associated with “DVT unlikely" (5% prevalence of DVT). These patients should proceed to D-dimer testing. A score of 1 to 2 is considered moderate risk, with a pretest probability of 17%. These patients should proceed to high-sensitivity D-dimer testing, as moderate-sensitivity D-dimer is not sufficient. A score ≥ 3 suggests DVT is likely. Pretest probability is 17% to 53%. All patients found to be “DVT likely” should receive a diagnostic ultrasound.
There is an low prevalence of DVT in patients with low clinical suspicion (< 25%). The Wells score inherently incorporates clinical gestalt, with a -2 score assigned when an alternative diagnosis is more likely than DVT. Sequelae from DVT include pulmonary embolism (PE) and pulmonary hypertension, which have an associated mortality of 1% to 8%. Anticoagulation is the mainstay treatment for DVT, although anticoagulation has its own associated risks of bleeding.
As with all clinical decision aids, the Wells criteria for DVT are meant to aid clinical decision making and not to force management. The criteria should be applied only after a detailed history and physical examination are performed. Likewise, the tool should be applied only to those patients who have been deemed to be at risk for DVT. If there is no concern for DVT, then there is no need for risk stratification.
Benjamin Slovis, MD
The Wells criteria for DVT were derived from a number of studies by Wells et al (Wells 1995, Wells 1997, Wells 2003) in an attempt to stratify risk for DVT in symptomatic outpatients. At the time, the clinical diagnosis of DVT was thought to be inaccurate, leading to widespread overuse of confirmatory imaging.
In their 2003 study, Wells et al identified 1096 outpatients with concern for DVT and randomized them into 2 groups after applying the Wells criteria for DVT. The control group of 520 patients had an ultrasound performed. The other group of 562 patients had D-dimer testing performed. If the D-dimer was positive, they also received an ultrasound; if the D-dimer was negative, no ultrasound was performed. Sixteen percent of the patients in the control group and 15.5% in the test group had DVT or PE, resulting in an overall prevalence of 15.7%. Among the 520 control patients, 279 were considered DVT-unlikely and 241 were considered DVT-likely. Sixteen (5.7%) of the DVT-unlikely patients had DVT or PE. In the control group overall, 6 patients (1.4%) who had been initially ruled out had a diagnosis of DVT on 3-month follow-up. Of the 562 patients in the D-dimer group, 315 were considered unlikely to have DVT and 247 were considered likely to have DVT. Seventy-one patients (28.7%) in the likely group had DVT. In the unlikely group, 38.8% of patients had a negative D-dimer and did not undergo further testing. Two of these patients (0.4%) had confirmed DVT on days 4 and 14 of follow-up. The negative predictive value of D-dimer was 96.1%. This algorithm was then supported by Scarvelis and Wells (Scarvelis 2006).
In 2006, Wells et al performed a systematic review (Wells 2006), which evaluated 8239 patients in 14 studies that used the Wells score to predict risk of DVT, and evaluated for the incidence of DVT in association with moderate- or high-sensitivity D-dimer. This review has been utilized by the American College of Chest physicians to provide guidelines for the evaluation of DVT.
The Wells score is less useful in hospitalized patients than in outpatient settings (Silveira 2015). There are several versions of these criteria with minor differences based on the study. The calculator on MDCalc uses the most widely validated criteria, based on the study by Wells et al in 2003 (Wells 2003).
Phil Wells, MD, MSc
Original/Primary Reference
Validation References
Additional References
Price: $75
+4 Credits!
Shane R. Sergent, DO, FAAEM, FACOEP, FAWM, RDMS; Michael Galuska, MD, FACEP, FAAEM; John Ashurst, DO, MSc, FACEP, FACOEP
Jennifer Maccagnano, DO, FACEP, FACOEP; Laura Melville, MD, MS
October 1, 2020
November 1, 2023
4 AMA PRA Category 1 Credits™, 4 ACEP Category I Credits, 4 AAFP Prescribed Credits, 4 AOA Category 2-A or 2-B Credits.
Accredited By





Our Partners


 678-366-7933
678-366-7933
